Legionnaires' Disease in Denmark 2025
Legionnaires' Disease in Denmark 2025
In 2025, 227 cases of Legionnaires' disease (LD) were registered among persons residing in Denmark, Table 1. Of these, 150 were men (24–96 years old, median age 69 years) and 77 were women (32–101 years old, median age 70 years). Of all LD cases, 19 (8.4%) died, of whom 12 were men (8%) and 7 were women (9.1%), within 30 days after disease onset or hospitalization, Table 1. The mortality rate was slightly lower than in 2024 and considerably lower than during the COVID-19 pandemic; see the annual report for 2024. For persons infected in Denmark, an overall decrease in the notification rate from 4.0 to 2.8 was observed from 2024 to 2025, with the largest decrease in the Copenhagen surrounding area, where the rate fell from 6.3 to 1.7, Table 2.
A total of 45 written reminders were sent regarding missing clinical notifications for cases with a test date in 2025. This subsequently resulted in the reporting of 27 cases to the Danish Health Data Authority's Electronic Reporting System (SEI2), while for 18 cases no notification was still received. It is unknown whether this was due to the absence of clinical pneumonia.
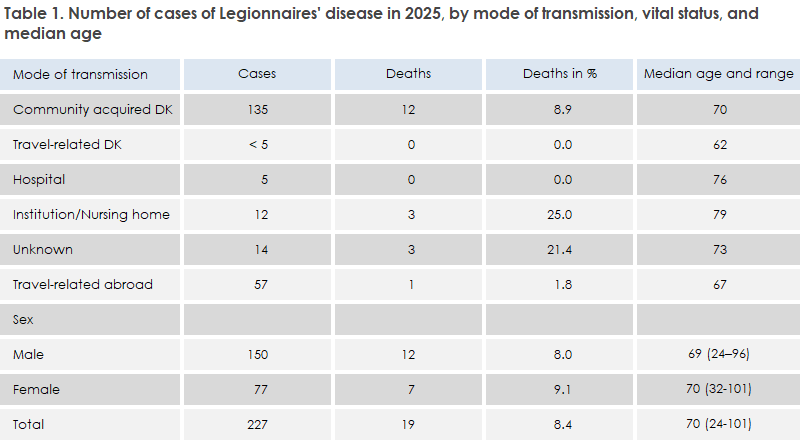
The proportion of LD cases aged ≥ 70 years remains high (50.2%), although it has been decreasing since 2022. Mortality in this age group has also declined since 2022 and was 14.9% in 2025; see the annual report for 2022.
The number of travel-associated cases (abroad) was largely unchanged compared with 2024 (57 vs. 56 cases), but the proportion increased from 18.9% in 2024 to 25.1%. These cases have a very low mortality rate (1.8%) and occur among somewhat younger persons than the remaining cases in other infection categories, Table 1. The ratio of men (n = 44) to women (n = 13) among the travel-associated cases resulted in an unusually high male-to-female ratio of 3.4:1 in 2025, whereas it normally lies around 2:1.
The sex distribution among persons infected in Denmark, including cases with an unknown infection category, was more evenly distributed, with a male-to-female ratio of 1.7:1, corresponding to the level in 2024 (1.4:1).
Infection in Denmark
A total of 170 of the registered disease cases in 2025, corresponding to 74.9%, are presumed to have been infected in Denmark when cases with an unknown infection category are included, Tables 1 and 2. This corresponds to a marked decline in the notification rate for domestically acquired cases compared with the previous four years, Table 2. Compared with 2024, the number decreased from 240 to 170 cases, corresponding to a decline of 29.2%.
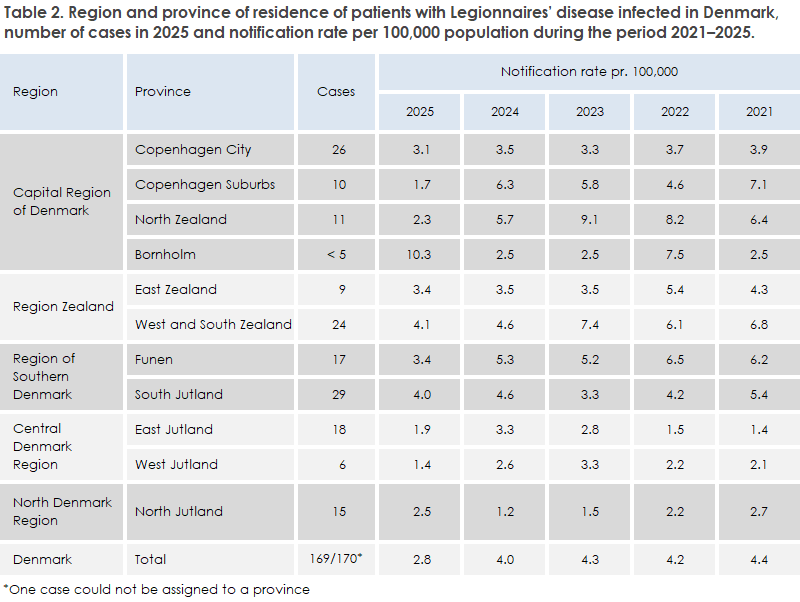
A large decrease in the number of cases was recorded in the Copenhagen suburbs and North Zealand provinces compared with the previous four years, Table 2. Together, the number of registered cases in these two provinces fell from 63 cases in 2024 to 21 cases in 2025, corresponding to a decrease of 66.7%. This decline accounted for 60% of the overall decrease for the entire country, corresponding to 42 out of a total of 70 fewer cases. In general, the notification rate declined in all provinces except North Jutland, where the rate increased from 1.2 to 2.5 per 100,000 inhabitants, and Bornholm, where the rate approximately quadrupled. However, Bornholm is particularly sensitive to fluctuations because of its small population base.
Community-acquired infection in Denmark
Of the 135 cases with community-acquired infection in Denmark, Table 1, 48 were culture-confirmed (35.6%). Of these, L. pneumophila serogroup 1 (SG1) was found in 23 patients (47.9%); among these, 10 were Pontiac and the remaining 13 were non-Pontiac. SG3 was found in 12 patients (25.0%). Among the remaining culture-confirmed cases, other L. pneumophila serogroups were detected in 11 patients, and L. bozemanae was detected in two patients.
Statens Serum Institut (SSI) is aware that, for 36 cases, one or more water samples were examined from the water supply in the patient’s own home and/or from another suspected source of infection. For 34 of the cases, the water samples were positive for L. pneumophila. Among 23 culture-confirmed L. pneumophila cases for which water samples had been collected, concordance between patient isolates and isolates from samples from the hot-water system in the patients’ own homes was found in eight cases.
In six of these eight cases, the strains involved were less virulent types: SG1 OLDA/Oxford (one case), SG1 Bellingham (one case), SG3 (one case), SG6 (two cases), and one non-typeable non-SG1 strain. In two cases, the more infectious type SG1 Benidorm ST42 was detected. Thus, the source of infection could only be verified in eight of the 36 investigated cases, and the infection circumstances therefore remain unresolved for the majority of LD cases presumed to have been acquired in Denmark.
Among the eight cases with a match between patient and water isolates, one case from 2025 formed part of a small cluster with the same type, SG1 Bellingham ST59, as a new case infected in 2026. Both patients live in the same building. In addition, one case was part of a long-standing cluster, known since 2006, associated with a large residential area with registered cases caused by SG1 Benidorm ST42. Two non-culture-confirmed cases were epidemiologically linked to another long-standing cluster, known since 2011, in a residential area where SG1 Philadelphia ST1 has been detected in patients, but never in water samples from the housing development. In addition, there were two other small clusters linked to the same buildings.
Infection during travels within Denmark
Fewer than five persons were presumed to have been infected while travelling within Denmark, partly during stays at campsites and partly in connection with stays at hotels. Among these were cases linked to a hotel from which a total of 11 cases have been registered since 2019, with SG1 Philadelphia ST1 detected in both environmental samples and clinical specimens.
Institution- and hospital-acquired infection in Denmark
Seventeen cases with presumed or confirmed infection acquired in healthcare institutions were reported: five from hospitals and 12 from other institutions such as nursing homes. For both groups, this represents a decrease compared with 2024, where nine and 28 cases, respectively, were identified. In total, six of these cases were culture-confirmed: two with L. pneumophila SG1 (one Pontiac and one non-Pontiac, respectively), three with other serogroups of L. pneumophila, and one case with L. anisa. The remaining cases were diagnosed exclusively by other methods. SSI is aware that water samples were examined from seven of the institutions/hospitals. In four of these cases, clinical isolates were available, but no match with the water samples was found in any of the cases.
Infection acquired during travel abroad
Infection abroad occurred in all months of the year, but most frequently in August with nine cases and November with eight cases.
A total of 57 persons (25.1%) were probably infected during travel abroad, Table 1, which is at the same level as in 2024. Italy was the most common country of travel with 10 cases, followed by Thailand with nine cases, Spain with seven cases, and the United Arab Emirates, including Dubai, with five cases. These are often the same countries associated with the highest numbers of cases, but in 2025 relatively more cases were registered among persons infected in Thailand and Spain than previously. Imported cases were recorded from a total of 22 different countries.
Of the 57 cases, 44 were reported to the European Centre for Disease Prevention and Control (ECDC) for preventive follow-up in the respective countries. The cases that were not reported were either associated with private accommodation, such as the person's own home abroad or visits to family, or with missing information on the place of stay during the incubation period; consequently, these cases could not be referred with certainty for preventive follow-up in the relevant countries.
Eleven of the travel-associated cases were part of eight international clusters involving at least two infected persons at the same hotel within a two-year period. Of these, three clusters were linked to hotels in Albania, Thailand, and Turkey, respectively, where each hotel had multiple Danish cases associated with it.
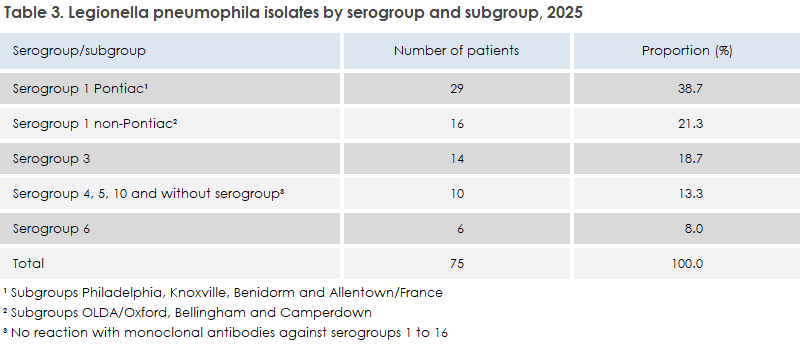
In total, 18 of the travel-related cases were culture-confirmed. Among these, L. pneumophila SG5 Dallas was detected in one case, and L. pneumophila SG1 was detected in 16 cases (88.9%), all of which belonged to SG1 Pontiac subgroups. These 16 cases accounted for 55.2% of all culture-confirmed SG1 Pontiac cases in 2025, Table 3. One case associated with travel to Thailand was culture-positive for L. longbeachae. It is well known that L. longbeachae is a relatively common cause of Legionnaires' disease in Thailand and Southeast Asia.
Sixteen cases of travel-associated Legionnaires' disease were LUT-positive, corresponding to 38% of all LUT-positive cases. Of these, six were diagnosed exclusively by LUT. Among these six cases, three were PCR-negative.
Laboratory confirmed cases by culture 2025
L. pneumophila was detected by culture in 75 patients. L. bozemanae was detected in two patients, while L. longbeachae, L. gormanii, and L. anisa were each detected by culture in one patient.
Thus, in 2025, 80 out of 227 cases were culture-confirmed (35.2%), which is a somewhat lower level than in the preceding three years. The distribution by serogroup and subgroup for L. pneumophila is shown in Table 3.
In addition to serogroup determination, the clinical L. pneumophila isolates were assigned a sequence type (ST) using whole-genome sequencing. A total of 42 different STs were identified. The most common ST was, as in previous years, ST1, which belonged to SG1, including both the Pontiac subgroup Philadelphia and the non-Pontiac subgroup OLDA/Oxford. ST1 was detected in 15 patients (20.0%), Table 4. This proportion is typical for Denmark, where ST1 usually accounts for 20–25% of cases, except in 2024 when the proportion was 14.5%. Among the domestically acquired cases, there were 14 ST1 cases, representing 24% of all culture-confirmed domestically acquired L. pneumophila cases. The second most common ST among domestically acquired cases was, as usual, ST87, belonging to SG3, with five cases. For 33 STs, across all infection categories, only a single case was associated with each ST.
Serogroup 3 accounted for a higher proportion in 2024 (27.3%) than in 2025 (18.7%), but the 2025 level was in line with 2022 and 2023, when the proportions were 19.8% and 17.1%, respectively. All SG3 cases are presumed to have been acquired in Denmark.
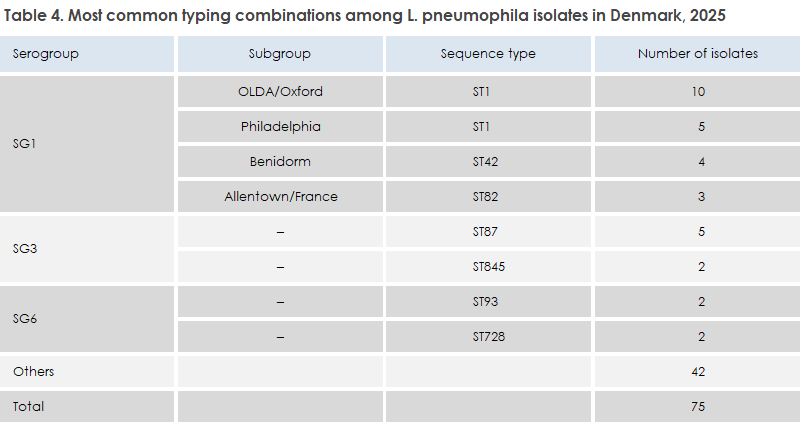
Table 4 shows the most common combinations of serogroup, subgroup, and sequence type (ST). Combinations associated with only a single LD case are grouped under “Other.”
Laboratory-confirmed cases detected by PCR and UAT in 2025
In 2025, 204 patients had a positive Legionella PCR test (89.9%). The L. pneumophila urinary antigen test (UAT), which predominantly detects SG1, was positive in 42 cases (18.5%). The number and proportion of UAT-positive cases were slightly higher than in 2024, but must still be considered to be at a very low level. A total of 23 cases were diagnosed solely on the basis of a positive UAT.
For travel-associated Legionnaires' disease, UAT generally has better sensitivity than PCR performed on respiratory specimens.
Of the 204 PCR-positive patients, 28 (13.7%) were positive either for non-L. pneumophila Legionella (n = 24) or for Legionella species (n = 4), where the latter four had not been tested for L. pneumophila. In addition to the five cases in which the species could be identified by culture, the species was determined in seven cases by sequencing the region between the 23S and 5S genes: L. longbeachae in two cases, and L. adelaidensis, L. beliardensis, L. feeleii, L. maceachernii, and L. rubrilucens in one case each.
In three regions—North Jutland, Central Jutland, and Zealand—as well as in the Funen area, PCR testing is performed exclusively for L. pneumophila. Therefore, some underdiagnosis of Legionnaires' disease caused by Legionella species other than L. pneumophila must be assumed in a substantial part of the country.
This report is also discussed in EPI-NEWS 24/2026.