No 24 - 2026
Legionnaires’ disease in Denmark 2025
Legionnaires’ disease in Denmark 2025
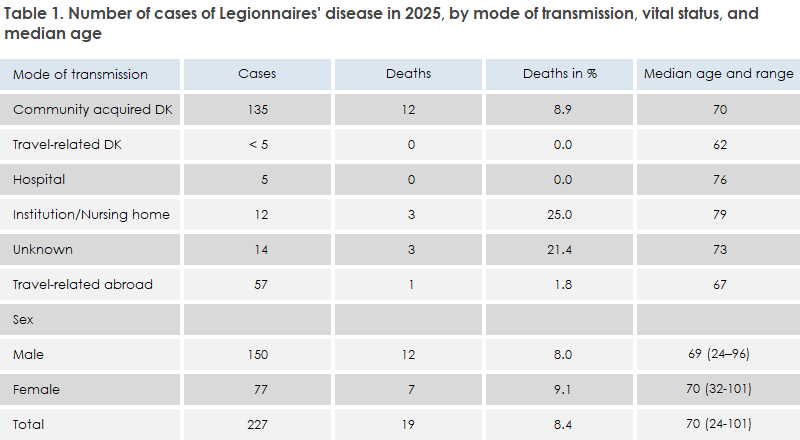
- In 2025, a total of 227 cases of Legionnaires’ disease (LD) were registered among persons residing in Denmark.
- In total, there were 150 men and 77 women, with a median age of 69 and 70 years, respectively.
- A total of 19 persons (8.4%) died within 30 days after disease onset or hospital admission.
- Among cases infected in Denmark (n = 170), the recorded incidence, calculated as the notification rate, was 2.8 cases per 100,000 inhabitants. This is a decrease compared with 2024, when 240 domestically acquired cases were registered, corresponding to a notification rate of 4.0 cases per 100,000 inhabitants.
- The majority of cases were assessed as having been infected in Denmark, while 57 cases (25.1%) were assessed as travel-related.
- Most domestically acquired cases, 59%, could be attributed to community-acquired infection in Denmark (Table 1). In the vast majority of these cases, the suspected and investigated source of infection was domestic water in the patient’s own home.
For a detailed epidemiological overview, see the 2025 annual report.
In the provinces Copenhagen Suburbs and North Zealand, a combined decrease was observed from 63 registered cases in 2024 to 21 cases in 2025, which accounted for 60% of the total decrease among all domestically acquired cases. This could not immediately be explained by fewer registered Legionella tests or by missing clinical notifications. It is therefore possible that the development reflects a real decline in disease incidence. The decrease in North Zealand is a continuation of a decline after 2023 (Table 2, 2025 annual report), when there was a very high rate of 9.1 cases per 100,000 population. A recent Danish study of Legionella diagnostics and surveillance during the period 2014–2022 showed that trends in the number of registered cases were closely associated with trends in the number of Legionella tests performed. The results underscore that changes in disease incidence should be interpreted in light of diagnostic activity, as both testing activity and clinical awareness can influence the number of registered cases.
For 36 domestically acquired cases, the source of infection was investigated through water sampling. In eight of these cases, the source of infection could be verified through concordance between water and patient samples. For the majority of domestically acquired cases, a specific source of infection could not be identified, which continues to complicate the assessment of the most important sources of Legionnaires’ disease in Denmark.
Travel
The number of travel-related cases of Legionnaires’ disease in 2025 was at the same level as in 2023 and 2024, but accounted for a larger proportion of the total cases compared with previous years.
Travel-related cases were registered from a total of 22 countries, particularly Italy (n = 10), Thailand (n = 9), Spain (n = 7), and the United Arab Emirates (n = 5). Several cases were associated with private travel or stays in private accommodation, which limited the possibilities for further source tracing.
During the past three years, nearly 60 people per year have contracted Legionnaires’ disease while traveling abroad. Infection most often occurs through inhalation of aerosols from water systems in which Legionella has had favourable growth conditions, typically due to lukewarm or stagnant water and inadequate temperature control or water circulation. In most travel-related cases, infection is assumed to originate from domestic or bathing water during stays at hotels or other accommodation facilities. However, infection can also occur from other sources, including hot tubs, cooling towers, misting devices, fountains, and other installations that generate water-containing aerosols.
Prevention
Preventive measures in travel-related settings include allowing the hot water to run from the shower and sink for a few minutes upon arrival, while leaving the bathroom to avoid inhaling aerosols. It may also be relevant to ensure that the hot water becomes so hot that you cannot keep your hand under it, as Legionella thrives particularly well in lukewarm water and at water temperatures below approximately 50°C. In older or poorly maintained installations, special attention should be paid to aerosol generation from hot water, especially during showering. The use of hot tubs should be avoided if hygiene conditions appear uncertain. These are also general preventive measures that can be applied after prolonged absence from one’s own home.
The risk of severe Legionnaires’ disease is particularly increased among older adults, smokers, and individuals with chronic diseases and/or impaired immune systems.
Legionella longbeachae
One travel-related case had stayed in Thailand and was diagnosed with infection caused by Legionella longbeachae. This species is a well-known cause of Legionnaires’ disease in Thailand, Southeast Asia, Australia, and New Zealand, and is often associated with exposure to compost, potting soil, planting soil, and soil-conditioning products during gardening and greenhouse work. In recent years, infections with L. longbeachae have been reported in increasing numbers in several Northern European countries. In 2025, two cases of L. longbeachae with presumed infection acquired in Denmark were registered, compared with 12 cases in 2024.
Infection can be prevented through good hygiene practices during gardening, such as wearing gloves, moistening dry potting soil or compost before handling it, and thoroughly washing hands and, if necessary, forearms with soap after completing the work. In addition, contact with the face and mouth should be avoided while gardening. The use of a dust mask, such as an FFP2 or FFP3 respirator, may also be considered when handling larger amounts of dry compost or potting soil, particularly in enclosed spaces such as greenhouses or sheds.
Clinical reports
Legionnaires’ disease is a clinically notifiable disease requiring individual case reporting. In 2025, 45 written reminders were issued regarding missing clinical notifications. This underscores the need for continued focus on clinical disease reporting to support disease prevention and ensure high data completeness in the national surveillance system.
S.A. Uldum, M.K.A. Holm, Bacteria, Parasites ad Fungi, C. Kjelsø, Department of Infectious Disease Epidemiology and Prevention