Integrated surveillance of respiratory infections in 2025/26 – consolidated report
Integrated surveillance of respiratory infections in 2025/26
The 2025/26 respiratory season was dominated by influenza
The 2025/26 respiratory season was characterized by high influenza activity. In addition, for the first time, an outbreak of influenza was observed outside the expected season.
In week 33 of 2025, a sudden increase was observed in the number of influenza A cases from around 20 cases weekly to 115 cases. Virological typing of the virus as well as interviews with a sample of the patients showed that it was an outbreak of influenza A(H1N1) at a music festival. During the following weeks, influenza activity again fell to a level corresponding to what is expected outside the season. Thus, the outbreak did not develop into an early season start.
In week 47, the influenza season began. The season was dominated by influenza A(H3N2) clade K, a virus that had changed after influenza strains had been selected for the vaccines. This meant that the 2025/26 season became a season with high influenza activity. But despite the changes in the circulating virus, vaccine effectiveness calculations showed that there was still an effect of the influenza vaccine.
New offer to pregnant women for vaccination against RSV
From 1 October 2025 to 31 January 2026, seasonal RSV vaccination was offered to pregnant women, EPI-NEWS 38/2025. During this period, pregnant women in weeks 32–36 of pregnancy could receive the vaccination free of charge. Uptake of the program was high: 72.7% of the children who were born between 1 November 2025 and 31 March 2026 had mothers who had accepted the offer of RSV vaccination. The high uptake was also reflected in the surveillance, where both the number of detected RSV infections and RSV-related hospitalizations among children aged 0–6 months were reduced compared with previous seasons, Figure 1.

Summary of the 2025/26 season
- Influenza: The season was characterized by high influenza activity, and from the end of 2025 onwards influenza was the most dominant respiratory infection—both measured by the number of infected individuals and hospitalized patients. For several weeks, both the number of cases and hospitalizations remained at a high level, and in some weeks the number of hospitalizations reached a very high level.
- COVID-19: The season was milder than previous seasons, as the number of cases and hospitalizations remained at a moderate level throughout 2025 and then fell to a low level in 2026.
- RSV: Overall, the RSV season was milder compared with previous seasons. The number of RSV cases and hospitalizations reached a high level in some weeks. The milder season is attributed to the fact that pregnant women were offered RSV vaccination from 1 October 2025 to 31 January 2026.
- Mycoplasma pneumoniae: The number of infections and hospitalizations was at a very low level in most weeks.
- Vaccination uptake: Influenza and COVID-19 vaccination uptake was 75% and 73%, respectively, among the older segment of the population aged 65 years and above.

Disease-specific data
Influenza
The 2025/26 influenza season was characterized by high activity, with the season beginning in week 47. Subsequently, both the number of cases and hospitalizations remained at a high level for several weeks, and the number of hospitalizations reached a very high level in some weeks, Figure 2. For the first time since influenza surveillance was established in Denmark, an outbreak was detected outside the influenza season, caused by influenza A(H1N1).
Influenza outbreak: In week 33 of 2025, 115 laboratory-confirmed influenza A cases were detected, which was almost six times higher than expected. Virological typing of viruses received through sentinel surveillance showed that these were identical influenza A subtype H1N1 viruses, which had also been the dominant virus at the end of the 2024/25 season. Following interviews with a sample of the patients, it became clear that this was an influenza outbreak at a music festival.
Circulating virus: Influenza A virus was dominant throughout the season. Subtype H1N1 was dominant at the start of the season, but the number of influenza A viruses of subtype H3N2 increased rapidly, and overall 2,543 (61%) influenza A subtype H3N2 viruses and 1,516 (36%) subtype H1N1 viruses were detected. Analysis of the genomes of the circulating H3N2 viruses showed that a specific genotype called subclade K was dominant and had changed compared with the vaccine strain. This genotype was also reported from other countries that experienced an early season start, figure 3. Few influenza B cases were detected, primarily during the latter part of the season, Figure 3.

Laboratory-confirmed cases: In 2025/26, influenza was detected in 21,829 individuals, of whom 21,486 had influenza A and 343 had influenza B. For comparison, influenza A or B was detected in 28,414 individuals in 2024/25 and 19,160 individuals in 2023/24, Figure 4. The highest influenza A incidence in 2025/26 was observed in the age group 85 years and older, followed by children aged 0–1 year.

Hospitalizations: In 2025/26, there were 7,855 influenza-related hospitalizations (36% of cases), which is higher than in previous seasons. A total of 7,790 of these were related to influenza A and only 65 to influenza B. For comparison, there were 7,128 influenza-related hospitalizations (25% of cases) in 2024/25 and 5,415 in 2023/24 (28% of cases). When comparing the proportion hospitalized in each age group with previous seasons, it is particularly among those aged 65 years and older that a larger proportion were hospitalized compared with earlier seasons.
Deaths: In 2025/26, there were 680 influenza-related deaths (3.1% of cases), which were primarily in the oldest age groups and related to influenza A, and slightly higher than in previous seasons.
For comparison, there were 583 influenza-related deaths in 2024/25 (2.1% of cases), 405 deaths in 2023/24 (2.1% of cases), and 274 deaths in 2022/23 (1.3% of cases).
Vaccination uptake: Uptake of influenza vaccination was again very high in 2025/26 among the older segment of the population, with 84% of nursing home residents and 75% of people aged 65 years and older being vaccinated. For comparison, uptake in 2024/25 was 85% among nursing home residents and 76% among people aged 65 years and older
Vaccine effectiveness: Influenza A(H3N2) clade K dominated during the 2025/26 season. This virus had undergone several changes after the influenza strains for the vaccines had been selected, which could affect vaccine effectiveness. In January 2026, estimates of vaccine effectiveness (VE), across vaccine types and age groups, showed that nearly half of influenza A cases could be prevented, VE = 45% (38–50%), as well as one quarter of hospitalizations, VE = 25% (14–34%).
It is well known that vaccine effectiveness wanes over the course of the season, and by the end of April 2026, when influenza activity was at a low level, estimates of VE across age groups and vaccine types showed that nearly one third of influenza A cases could be prevented, VE = 31% (26–35%), and nearly one fifth of hospitalizations, VE = 19% (13–24%).
Covid-19
Covid-19 does not follow the same seasonal pattern as influenza and RSV. During the last two seasons, elevated COVID-19 incidence has been observed in the second half of the calendar year, after which incidence declined to a low level following the turn of the year.
Circulating virus: At the beginning of the period and until December 2025, the recombinant XFG and its subvariants were dominant. Thereafter, BA.3 and its subvariants became dominant and have since remained among the most widespread variants, Figure 5. It is noteworthy that BA.3 is once again circulating in Denmark. The last time this variant was detected was in 2022. The graph presents data up to March 2026, after which there are insufficient sequencing data to describe developments.

Laboratory-confirmed cases and wastewater surveillance: In 2025/26, SARS-CoV-2 was detected in 6,127 individuals. For comparison, SARS-CoV-2 was detected in 12,345 individuals in 2024/25 and 24,943 individuals in 2023/24, representing a halving from year to year. In 2025/26, the number of laboratory-confirmed cases did not rise above a moderate level, Figure 2.
Wastewater-based surveillance of SARS-CoV-2 showed concentrations during the 2025/26 season at a level corresponding to the 2024/25 season, Figure 6, but with a higher concentration at the seasonal peak (week 32 to the turn of the year), reflecting a higher degree of transmission in the community during that period. Levels in both seasons were lower than in the preceding three seasons. Overall, there was good agreement between trends in wastewater surveillance and laboratory-confirmed cases.

Hospitalizations: In 2025/26, there were 2,814 SARS-CoV-2-related hospitalizations (46% of detected cases), which is in line with previous seasons. For comparison, there were 5,522 SARS-CoV-2-related hospitalizations (45% of cases) in 2024/25 and 10,179 SARS-CoV-2-related hospitalizations (41% of cases) in 2023/24. In all three periods, the highest SARS-CoV-2-related hospitalization incidence was observed in the oldest segment of the population, those aged 80 years and older.
Vaccination uptake: Uptake of COVID-19 vaccination was again very high in 2025/26 among the older segment of the population, with 84% of nursing home residents and 73% of people aged 65 years and older being vaccinated. For comparison, vaccination uptake in 2024/25 was 85% among nursing home residents and 75% among people aged 65 years and older.
Vaccine effectiveness: Among individuals aged 65 years and older who were offered seasonal COVID-19 vaccination during the 2025/26 season, there was good and relatively sustained protection against COVID-19-related hospitalization and death during the period from 1 October 2025 to 31 January 2026. The vaccine had an effectiveness of 61% (48–70%) and 70% (54–81%) against COVID-19-related hospitalization and death, respectively. A decline in protection against hospitalization was observed during the first four months after vaccination, from 66% (48–78%) immediately after vaccination to 48% (10–71%) in the fourth month following vaccination. It should be noted, however, that the confidence intervals are wide, particularly for the latter estimate. No significant decline in protection against death was observed within four months after vaccination.
Respiratory syncytial virus (RSV)
The 2025/26 RSV season began in week 50, Figure 2, which is later than the previous post-pandemic seasons. At the same time, activity was lower both in terms of the number of cases, Figure 7, and hospitalizations, Figure 1. This is attributed to RSV vaccination of pregnant women aimed at protecting infants during their first months of life.

Circulating virus: As in the previous season, the 2025/26 season showed an almost equal distribution of RSV A (645 detected cases, 45%) and RSV B (808 detected cases, 55%). However, RSV B became more dominant during the latter part of the season, Figure 8.

Laboratory-confirmed cases: In 2025/26, RSV was detected in 5,524 individuals. For comparison, RSV was detected in 8,309 individuals in 2024/25, 10,117 individuals in 2023/24, and 11,924 individuals in 2022/23. The reduction in the number of cases from 2024/25 to 2025/26 was greatest in the youngest age groups. The number of cases among infants aged 0–3 months decreased from 1,215 cases to 372 cases (69% fewer cases), and among infants aged 4–6 months from 512 to 253 cases (50% fewer cases).
Hospitalizations: During the 2025/26 season, 2,202 RSV-related hospitalizations were recorded, corresponding to 40% of all cases. For comparison, 2,831 RSV-related hospitalizations were recorded in 2024/25 (34% of all cases), 3,252 hospitalizations in 2023/24 (32% of cases), and 5,135 in the 2022/23 season (43% of cases). The reduction in RSV-related hospitalizations from 2024/25 to 2025/26 was greatest in the youngest age groups. Hospitalizations among infants aged 0–3 months decreased from 710 cases to 223 cases (69% fewer hospitalizations), and among infants aged 4–6 months from 172 to 105 hospitalizations (39% fewer hospitalizations).
In previous seasons, hospitalization incidence was highest among infants aged 0–5 months. However, in 2025/26 it was highest among individuals aged 75–84 years.
Deaths: In the 2025/26 season, there were 128 RSV-related deaths (2.3% of cases). For comparison, there were 117 RSV-related deaths in 2024/25 (1.4% of cases), 109 deaths in 2023/24 (1.1% of cases), and 290 deaths in 2022/23 (2.4% of cases). In all seasons, deaths occurred predominantly in the oldest age groups.
Vaccination uptake: From 1 October 2025 to 31 January 2026, RSV vaccination was offered to pregnant women in weeks 32–36 of pregnancy. Uptake of the program was high: 72.7% of children born between 1 November 2025 and 31 March 2026 had mothers who accepted the offer of RSV vaccination.
Mycoplasma pneumoniae
Throughout the 2025/26 season, M. pneumoniae circulated at a very low to low level, Figure 2. This low level was expected following the M. pneumoniae epidemic that lasted from autumn 2023 to spring 2025, Figure 9.

Laboratory-confirmed cases: In 2025/26, M. pneumoniae was detected in 641 individuals. For comparison, M. pneumoniae was detected in 40,742 individuals in 2024/25 and in 14,636 individuals in 2023/24.
Hospitalizations: In 2025/26, 119 M. pneumoniae-related hospitalizations were recorded, corresponding to 19% of cases. For comparison, 2,982 M. pneumoniae-related hospitalizations were recorded during the 2024/25 season, corresponding to 7% of all cases. During the 2023/24 season, 1,608 patients (11%) were hospitalized in relation to a M. pneumoniae infection.
Sentinel surveillance monitors a range of respiratory viruses
The sentinel surveillance system is based on reports from general practitioners (GPs) and operates as a voluntary, sample-based reporting system that monitors influenza, COVID-19, and other respiratory virus infections.
During the 2025/26 season, 93 general practices participated in the surveillance. Sentinel physicians report weekly how many patients with influenza-like illness (ILI) they see in their practices, as well as the total number of consultations conducted during the same week.
The consultation percentage remained at a low level throughout autumn 2025 but increased to a moderate level from week 41. From week 47, the consultation percentage increased further and reached a high level in week 52 and again around week 5 of 2026. From week 7 onwards, the consultation percentage gradually declined and has remained at a low level since week 16. However, the marked increase in week 52 is considered to have been partly influenced by the holiday period, with fewer scheduled consultations and fewer reports submitted, which may result in an elevated consultation percentage, Figure 10.
It should be noted that the consultation percentage is not specific to influenza virus but also includes other respiratory infections where patients present with influenza-like illness in primary care.

Sentinel physicians also submit swab samples from a subset of patients with ILI. The season was characterized by a small SARS-CoV-2 wave beginning in the summer of 2025. Parainfluenza viruses and entero-/rhinoviruses dominated during the summer and into the autumn months. Thereafter, influenza and RSV accounted for the majority of cases. As in previous seasons, an increase in parainfluenza viruses was observed as influenza incidence declined, along with an increase in human metapneumovirus after the turn of the year in 2026.
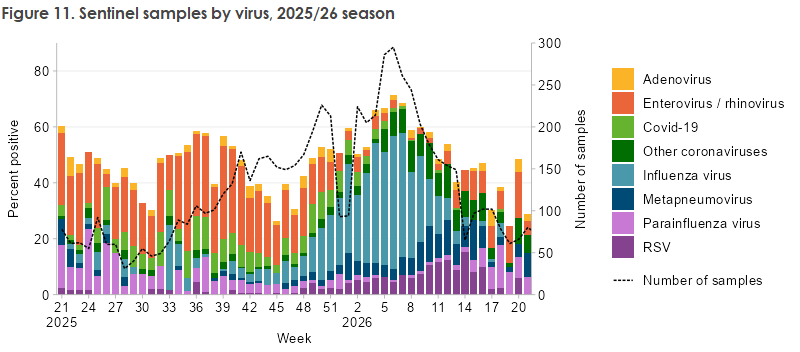
During the 2025/26 season, SSI received 5,153 sentinel swab samples from week 40 of 2025 through week 20 of 2026. Of these samples, 2,736 (38%) tested positive for at least one respiratory virus. The following viruses were detected: 117 adenoviruses, 254 RSV infections, 492 entero-/rhinoviruses, 270 endemic coronaviruses, 188 SARS-CoV-2 infections, 253 human metapneumoviruses, 130 parainfluenza viruses, and 1,032 influenza viruses. Compared with the previous season, fewer cases of all viruses were detected, with the exception of human metapneumovirus. The number of metapneumovirus detections was slightly higher than in the previous season despite a lower number of sentinel samples. The distribution of respiratory viruses among sentinel samples is shown in Figure 11.
Influmeter and surveillance via on-call physicians service
Influmeter is operated by Statens Serum Institut and is part of the European collaboration InfluenzaNet, which includes 11 countries with similar systems. The system complements the existing surveillance of influenza-like illness in Denmark. It is based on voluntary participation by members of the public, who report each week whether they have experienced symptoms—regardless of whether they have had contact with the healthcare system. In this way, participants contribute to a better understanding of the spread of influenza-like illness in the population.
During the 2025/26 season, approximately 3,300 individuals were enrolled, and around 2,000 submitted symptom reports each week. The results showed, similarly to the sentinel surveillance system, two periods of elevated ILI incidence (November–December and February). Among Influmeter participants, these periods were primarily driven by the 30–39-year age group, followed by those aged 40–49 years, Figure 12.

Influenza-like symptoms are also monitored through the on-call physicians service , and this surveillance operates year-round. In this system, on-call physicians across the country have the option to indicate whether a patient presents with influenza-like symptoms. The reported ILI consultation percentage follows the trends observed in the other surveillance systems, although with some variation between regions. The Capital Region of Denmark and Region Zealand reported an increasing incidence of ILI from week 47 onwards, whereas the other regions did not report a similar increase until after the new year (Figure 13).

This annual report is also described in EPI-NEWS 23/2026.