Imported cases of dengue fever in Denmark, 2010-2025
Imported cases of dengue fever in Denmark, 2010-2025
Dengue fever is a mosquito-borne viral disease that occurs endemically in tropical and subtropical areas and has increased globally in recent years. WHO estimates that around 96 million symptomatic cases and 40,000 deaths occur globally each year. In Denmark, dengue occurs only as an imported infection among travellers. In the period 2010-2025, a total of 1,039 laboratory-confirmed cases were registered in MiBa. Considerable variation is seen over the years, with a marked decline during the COVID-19 pandemic. Among cases for which information on country of travel is available, the majority appear to have been acquired in Asia, particularly in Thailand, Indonesia and India. The increase probably reflects both increased travel activity and increased local occurrence of dengue in endemic areas.
Since November 2023, dengue fever has been notifiable from diagnostic laboratories in Denmark to Statens Serum Institut (SSI), which monitors its occurrence. This report describes the number of imported dengue cases in the period 2010-2025 and the available travel information.
Dengue fever
Dengue fever is a viral infection caused by dengue virus (DENV), which occurs as four serotypes (DENV 1-4). DENV is transmitted to humans by bites from the mosquitoes Aedes aegypti (the yellow fever mosquito) and Aedes albopictus (the tiger mosquito). Changes in climatic and environmental conditions and urbanisation have contributed to the spread of the vectors to new geographical areas and thereby increased the risk of local transmission, also in non-endemic areas such as Europe, where the tiger mosquito is increasingly observed.
Most travellers who become infected with dengue do not experience symptoms. It is estimated that approx. 20% of infected persons become ill with milder symptoms such as fever, nausea, headache, joint pain and possibly a skin rash. Symptoms last approx. 1-2 weeks. In fewer than 1% of infected persons, more severe disease with a tendency to bleeding and risk of organ failure may occur. There is no specific antiviral treatment for dengue; treatment is symptomatic only (primarily rehydration therapy) and, in severe cases, may require hospitalisation. For a more detailed description of dengue, please also see SSI's Disease Dictionary under Dengue fever . For travellers to areas where dengue occurs, prevention is important and mainly consists of avoiding mosquito bites. In Denmark, the dengue fever vaccine Qdenga is approved, but as a general rule the vaccine is recommended only for travellers who have previously been infected with dengue and only for persons aged 6 to 60 years. See more about dengue vaccination in EPI-NEWS 7-9/2025 .
Laboratory diagnostics and case definition
Dengue virus can be detected by several laboratory diagnostic methods. In current diagnostics, serotypes are not routinely distinguished.
In the first days of illness, the diagnosis can be made by detecting viral RNA using RT-PCR. Viral RNA can typically be detected during the first week after symptom onset. During this period, it is usually also possible to detect dengue virus antigen.
Detection of DENV-IgM and possibly DENV-IgG in a blood sample indicates current or recent infection, but antibodies may be absent in the first days of illness. The serological diagnosis should therefore, where possible, be confirmed by testing paired blood samples to demonstrate a titre increase or seroconversion. Information on previous vaccination against dengue virus or another flavivirus is relevant for interpretation of the test result.
In this report, a 'confirmed case' of dengue is defined in accordance with ECDC's case definition as detection of DENV RNA, DENV antigen, detection of DENV-IgM confirmed by neutralisation test, or a fourfold titre increase in paired blood samples. As the false-positive rate for the above-mentioned tests is low, these laboratory results can stand alone without detailed information on the patient's symptoms and travel history.
A 'probable case' of dengue is defined as detection of DENV-IgM in a blood sample. However, false-positive IgM test results may occur. In addition, for probable cases there must be information on febrile illness and documentation of a stay in an area with current occurrence of dengue within two weeks before symptom onset. Because of the possible false-positive IgM test results, and because the Danish Microbiology Database (MiBa) does not contain information on symptoms and contains travel information only to a limited extent, only confirmed cases of dengue are included in this report.
Number of imported dengue cases in Denmark, 2010-2025
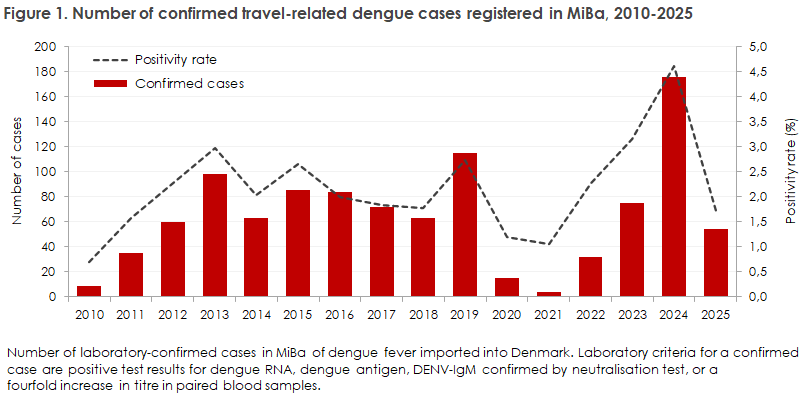
In the period 2010-2025, a total of 1,039 confirmed cases of dengue were registered in Denmark. The number of cases per year is shown in Figure 1. During the period, there was an average of 65 cases annually, varying from 4 to 175 cases per year. It may be noted in parentheses that 594 probable cases were detected in the same period, corresponding to an average of 37 cases per year, but these are uncertain and cannot be assessed further.
The number of imported confirmed dengue cases varied considerably during the period. From 2010 to 2013, a steady increase was observed, followed by a period from 2013 to 2018 with a relatively stable occurrence of between approx. 60 and 80 cases annually. In 2020-2021, a marked decline was seen in both the number of cases and testing activity, reflecting the decline in international travel activity during the COVID-19 pandemic.
From 2022, the number of cases increased again, with a pronounced increase in 2024, when both the highest number of cases and the highest positivity rate in the period were recorded. This increase did not continue in 2025, when the number of confirmed cases fell from 175 to 54.
The actual number of Danish travellers infected with dengue is expected to be higher than the number registered. This is due, among other things, to underreporting of mild or asymptomatic infections, and to cases where the course of illness has ended before return to Denmark and is therefore not diagnosed or registered in the Danish healthcare system.
Travel activity, age and sex distribution among infected persons
Travel activity is not registered systematically in MiBa in connection with testing for dengue virus. For the majority of cases, information on country of infection is therefore not available, which limits the possibilities for a precise geographical risk assessment.
For the period before 2016, travel information is available for only a few cases. Since then, information on travel destination has more often been provided as free text in requisitions from clinicians.
Overall, travel information is available for 33% of cases in the entire period. In all these cases, travel to destinations outside Europe was stated. If several travel destinations were stated for the same patient, the first stated country was registered as the country of infection. The geographical distribution of cases with known travel information is shown in Figure 2.
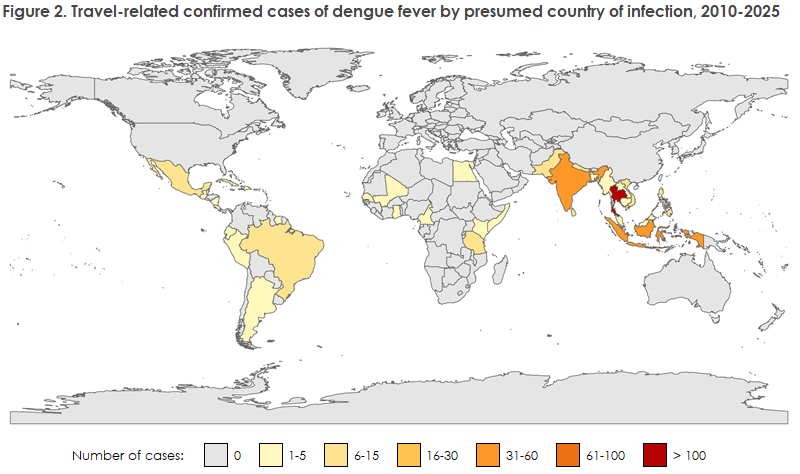
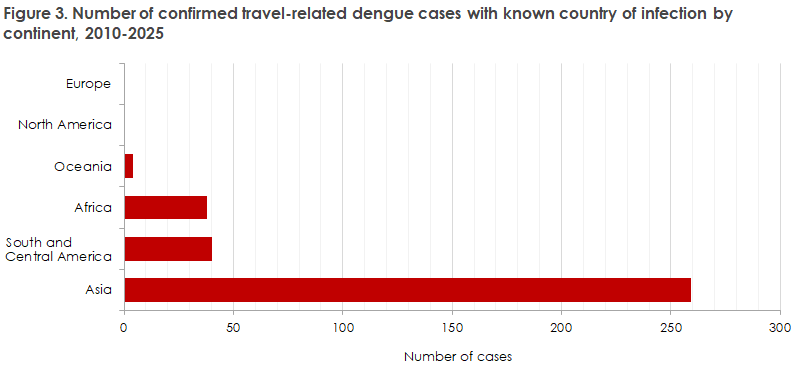
Asia is the most frequent region of infection throughout the study period, with a total of 259 confirmed cases. A total of 40 cases were registered from South and Central America, 38 from Africa and 4 from Oceania. No travel-related dengue cases from Europe or North America were reported, Figure 3.
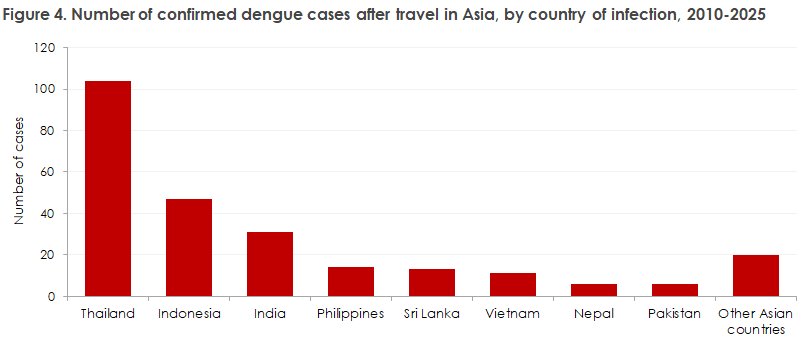
Within Asia, Thailand is the most frequently reported country of infection, with more than 100 cases. This is followed by Indonesia (47 cases) and India (31 cases). Asian countries with more than six cases during the period are shown as separate categories in Figure 4, while countries with fewer cases are grouped under 'Other Asian countries'.
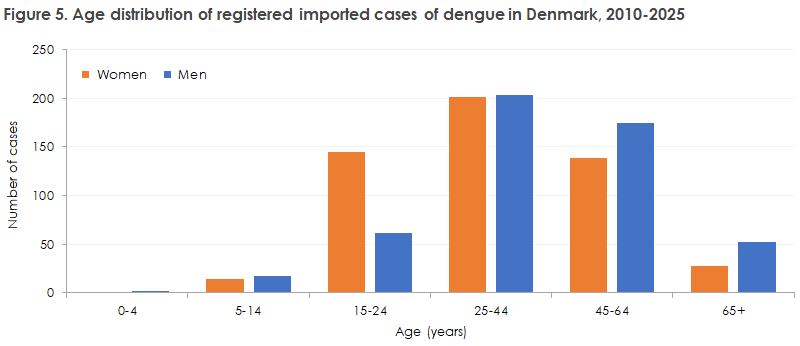
The distribution of laboratory-confirmed dengue cases by age and sex shows that most cases occur among adults of working age, particularly in the age group 25-44 years. Overall, the sex distribution is even, Figure 5. In the age group 15-24 years, however, there is a predominance of women, while in the older age groups (25-44 years, 45-64 years and >=65 years) there is a predominance of men. Relatively few cases are registered among children (0-14 years) for both sexes. This may reflect milder symptoms in children, but the observed age and sex distributions probably also reflect differences in travel activity to dengue-endemic areas.
This report is also described in EPI-NEWS 18b/2026.