Chlamydia – Occurrence of disease, 2025
Chlamydia – Occurrence of disease, 2025
Data from the Danish Microbiology Database
As in previous years, the data used for the preparation of the present report for 2025 were obtained through the Danish Microbiology Database (MiBa). The data comprise all positive and negative test results for oculo-genital infection caused by Chlamydia (C.) trachomatis from all departments of clinical microbiology (DCMs). The data include personal identification numbers, making it possible to define disease episodes at the individual level. A new disease episode is defined as an interval of more than 42 days between two sampling episodes with positive results. For patients with a valid personal identification number, information on municipality code and thereby province and region are obtained from the Civil Registration System.
Throughout the report, numbers from 2024 are presented for comparison. In 2024, the method by which chlamydia data are obtained from MiBa was revised and updated as part of a broader effort to standardise data extraction. The main difference between the two methods is that individuals may have more than one negative sampling episode per year, resulting in a higher number of testing episodes and thereby affecting positivity rates for the years before 2023. Consequently, the new method yields lower positivity rates than the previous method (by 1.3–2.3 percentage points). In the present report, the number of testing episodes from 2014 to 2025 is presented.
Other data
An unknown number of chlamydia tests are performed in private laboratories. Such data are not included in the present report. In cases where chlamydia is detected in rectal samples, or when lymphogranuloma venereum (LGV), EPI-NEWS 20/2008, is suspected, some DCMs and venereology clinics submit specimens to Statens Serum Institut (SSI) for specialised LGV testing.
Occurrence of chlamydia
In 2025, a total of 266,561 individuals (182,315 females, 84,068 males, and 178 individuals of unknown sex) were tested for chlamydia, corresponding to 331,795 testing episodes (Table 1), representing a decrease from 277,862 individuals tested and 352,378 testing episodes in 2024. The number of detected cases in 2025 was 29,580, which was unchanged compared with 2024, when 29,946 cases were recorded. The positivity rate increased from 8.5% in 2024 to 8.9% in 2025, but remained lower than that observed during the period 2014–2023. Not all tested individuals had information available on sex, age, and province of residence; consequently, different positivity rates may be observed in the following tables.
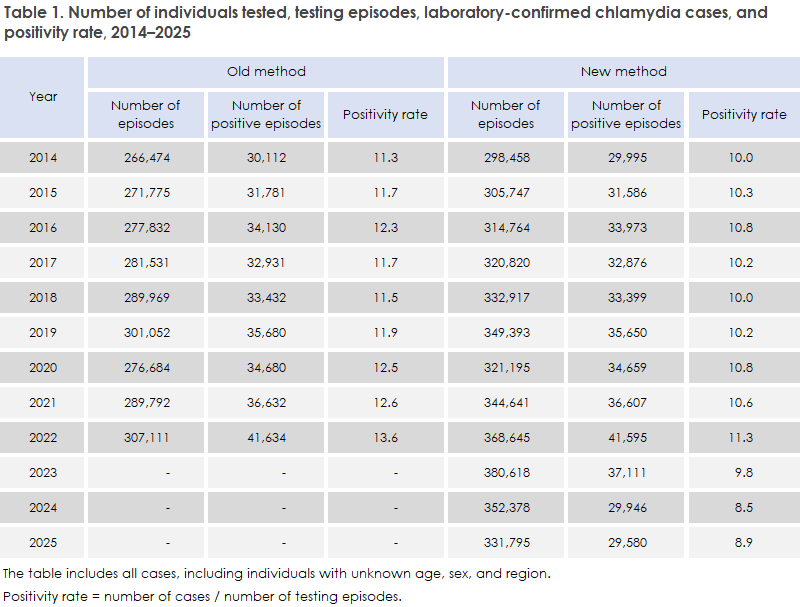
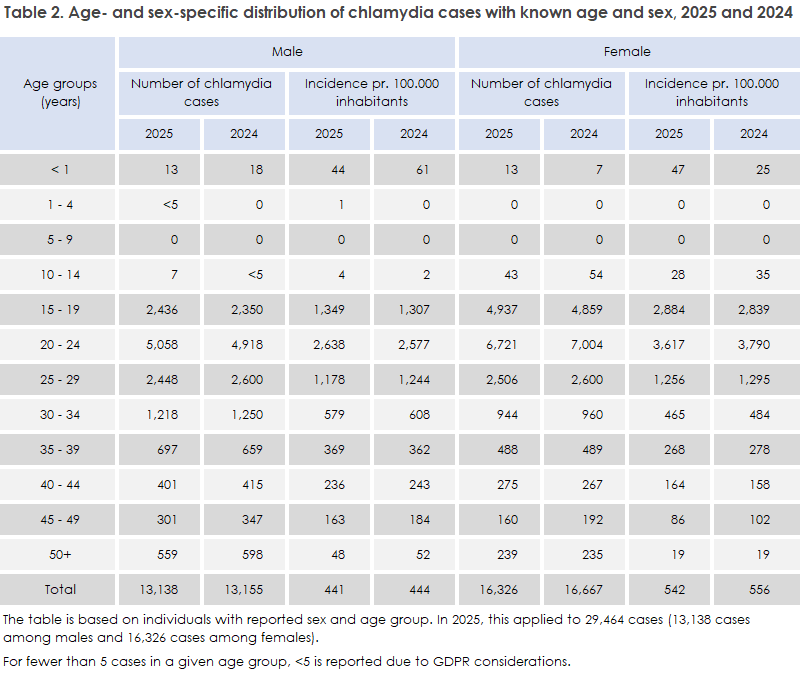
Table 2 is stratified by sex and shows the number of chlamydia cases and the incidence rate per 100,000 population. No major decreases or increases were observed among either males or females across the age groups. Overall, the age-specific distribution of chlamydia cases in 2025 was similar to that observed in 2024. A small decrease was observed among females aged 10–14 years, while the largest decrease was seen among persons aged 45–49 years, where the incidence rate declined by 11% among males and 16% among females, respectively. Overall, no change in the incidence rate was observed among either males or females from 2024 to 2025 (Table 2).
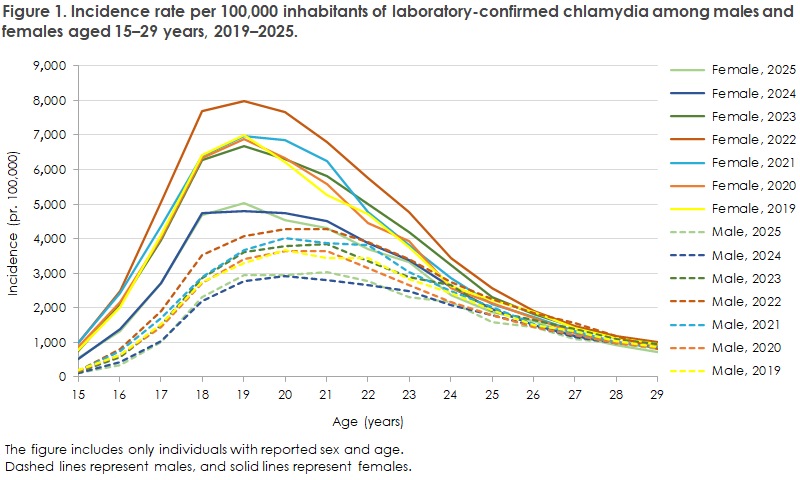
Among 15–29-year-olds, the incidence rate of detected chlamydia cases was unchanged from 2024 to 2025 (Figure 1). This means that, as in the previous year, this age group continued to exhibit the lowest incidence rates overall. Among females, the lowest incidence rate was observed among 19-year-olds, which has been the case for more than 10 years. Among males, the lowest incidence rate was observed among 21-year-olds, whereas in recent years the lowest rate has alternated between 20- and 21-year-olds. In 2025, 87% of all detected chlamydia cases among females occurred in the 15–29-year age group, while the corresponding proportion among males was 76%. Overall, 82% of all detected chlamydia cases occurred among 15–29-year-olds. In 2025, males accounted for 45% of all detected cases, representing an increase of one percentage point compared with 2024.
Geographical distribution
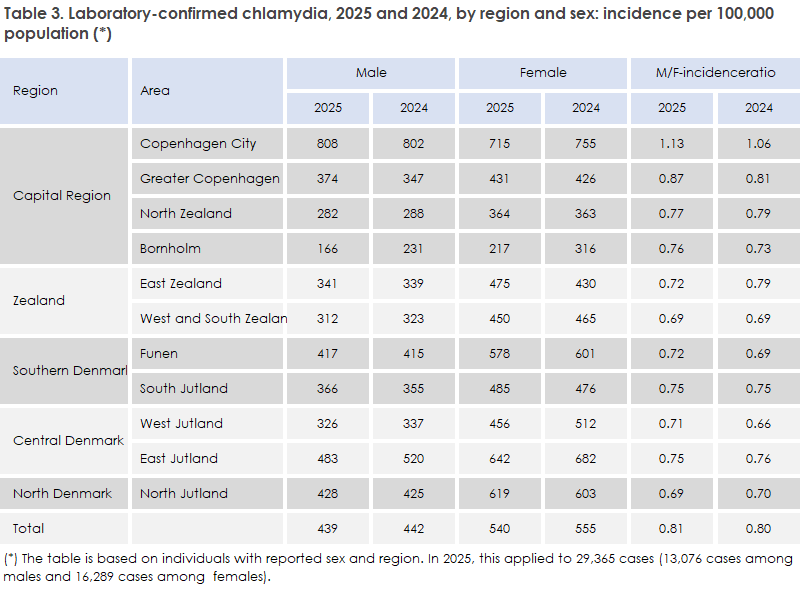
From 2024 to 2025, a decline in the incidence rate per 100,000 population was observed on Bornholm among both males and females, together with a small increase among females in East Zealand, Table 3. Otherwise, no major changes were observed in either incidence rates or the male-to-female (M/F) incidence ratio across the remaining part of Denmark. Copenhagen City was again the only area in which males had a higher incidence rate than females. The lowest M/F incidence ratio was observed in West and South Zealand and in North Jutland (0.69), whereas in 2024 the lowest ratio was observed in West Jutland (0.66). At the national level, the M/F incidence ratio remained unchanged in 2025 compared with 2024 (0.81 and 0.80, respectively) (Table 3).
Diagnostics
Among persons diagnosed with chlamydia in 2025, 90% had been tested by general practitioners or specialist physicians and 10% by hospital departments, unchanged from 2024.
Chlamydia in children
Chlamydia was detected in 77 children in 2025. Of these, 51 cases occurred among 1–14-year-olds and 26 among infants under one year of age. Twenty-five of the cases among infants were positive eye swabs. It is important to remember chlamydial infection as a cause of conjunctivitis in newborns.
Testing frequency by age group and sex
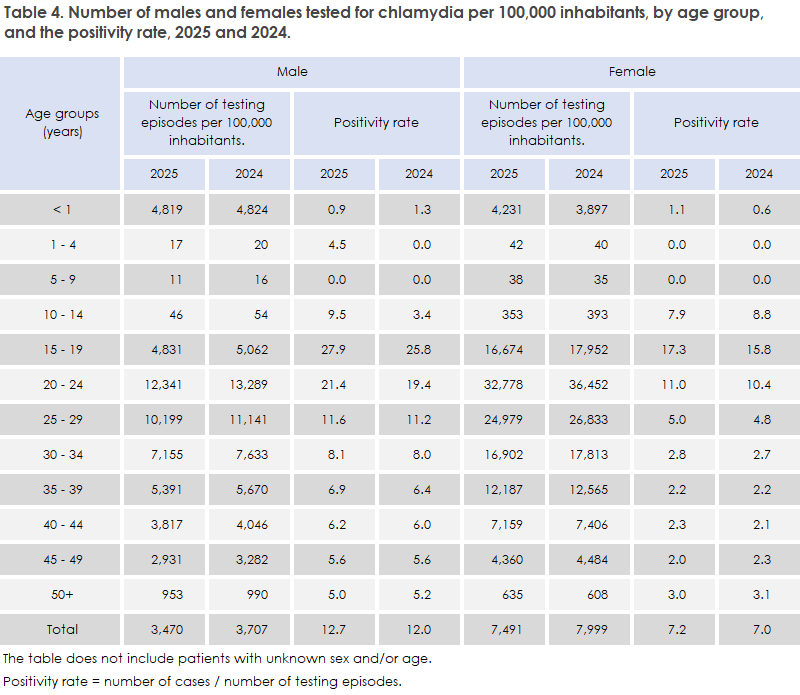
From 2024 to 2025, a continued overall decline was observed in the incidence rate of chlamydia testing, Table 4. However, a slight increase in this incidence rate was seen among females aged 50 years and older. The largest decline in the incidence rate of chlamydia testing was observed among 10–24-year-olds of both sexes and among males aged 45–49 years. In the 15–29-year age group, a slight increase in the positivity rate was observed despite declining testing activity. Among boys aged 10–14 years, a marked increase in the positivity rate was seen (3.4% in 2024 and 9.5% in 2025), whereas the positivity rate declined among girls in the same age group. The incidence rate of chlamydia testing decreased by 6% for both males and females. Overall, the positivity rate increased from 2024 to 2025 for both sexes, with the largest increases observed in the younger age groups (Table 4).
Treatment of chlamydia
In 2019, EPI-NEWS 38/2019, doxycycline was recommended instead of azithromycin for the treatment of uncomplicated chlamydia. The reason was the high prevalence of azithromycin resistance among Mycoplasma genitalium in Denmark compared with Sweden, where doxycycline is the standard treatment. Data from the Danish National Prescription Registry indicate that azithromycin use continues to decline but still accounts for approximately 40% of treatments in 2025. Its use should be reduced further.
In the 2024 chlamydia surveillance report EPI-NEWS 23–26/2025, it was incorrectly stated that azithromycin was used in approximately 60% of cases. The correct number should have been approximately 40% of cases.
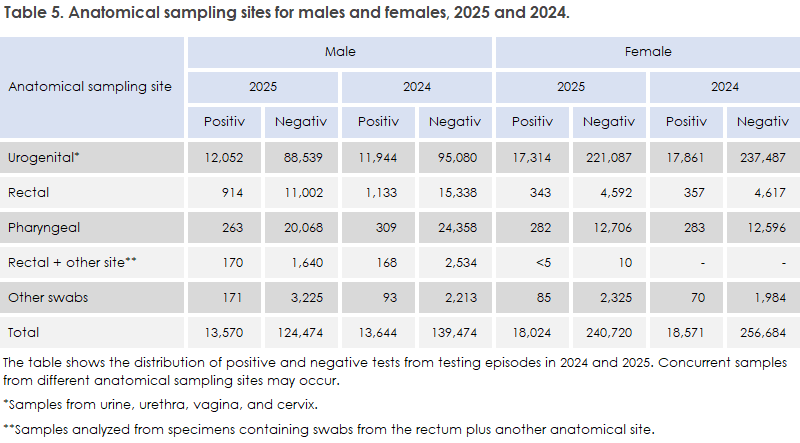
In 2025, no change was observed in the number of positive urogenital chlamydia tests among either males or females (Table 5). The number of rectal samples, including those classified as “rectal + other anatomical site”, from males with chlamydia decreased from 2024 to 2025. This may be attributable to the reduced screening activity among individuals receiving pre-exposure prophylaxis (PrEP) against HIV infection (Table 5).
Chlamydia testing and positivity rates by province and sex
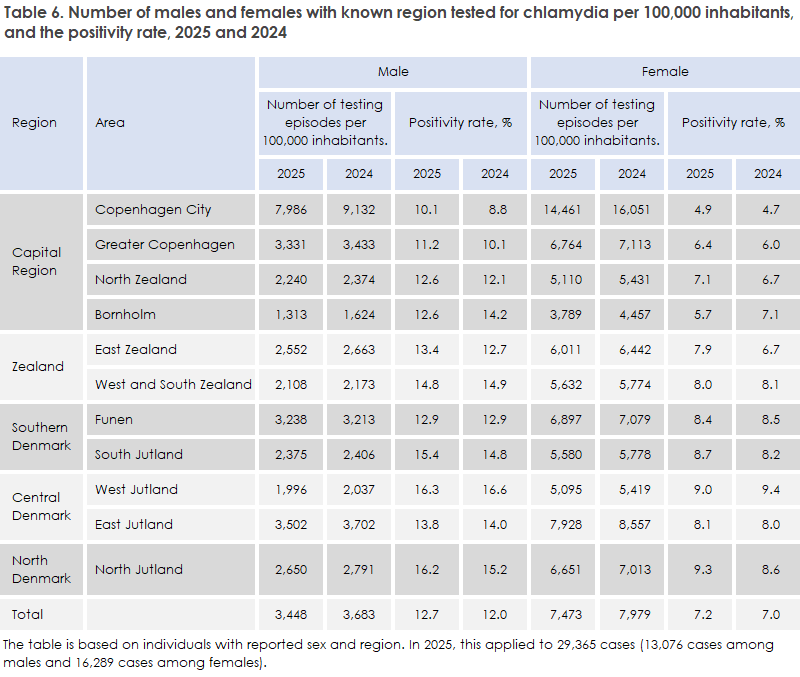
Overall, a decrease or no change was observed in the incidence rate of chlamydia testing across all provinces and in both sexes from 2024 to 2025 (Table 6). The positivity rate increased nationally, and in general increased across all provinces, with the exception of Bornholm, where a marked decline was observed in both the positivity rate and the incidence rate of testing. As in previous years, the highest incidence rate of chlamydia testing in 2025 was observed in Copenhagen City for both males and females, while the lowest incidence rate was again observed on Bornholm. West Jutland and North Jutland had the highest positivity rates among both males and females (16.3% and 9.0% in West Jutland, and 16.2% and 9.4% in North Jutland, respectively). In 2024, the highest positivity rate was observed in West Jutland.
Rectal chlamydia testing in males
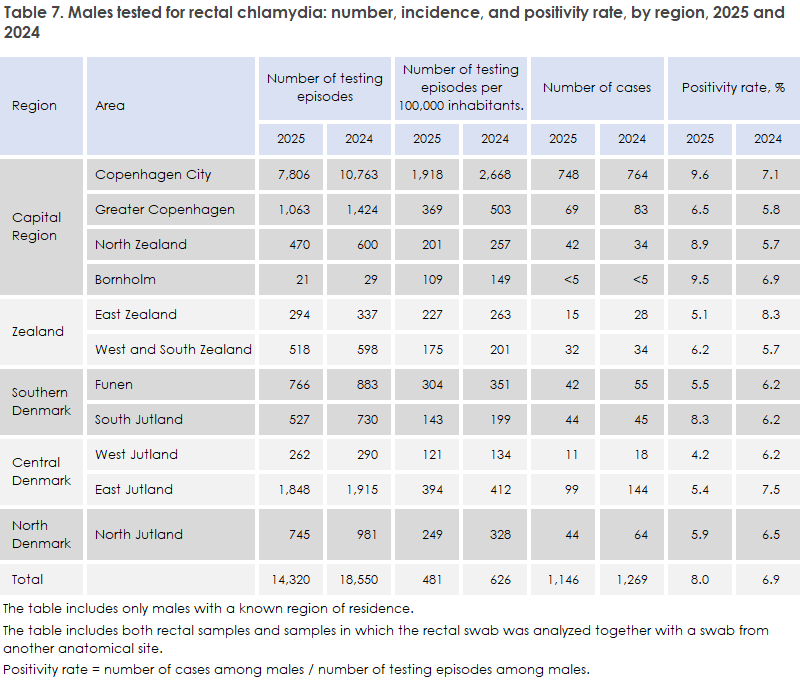
From 2024 to 2025, a decrease was observed in both the number of testing episodes and the number of detected cases, whereas the positivity rate increased across the country, with the exception of East Zealand, Funen, and West, East and North Jutland (Table 7). The table includes both rectal samples and samples in which a rectal swab was analysed together with a swab from another anatomical site, most often the pharynx. A decrease in the number of tests performed was observed in all provinces, particularly in Copenhagen City, where the number of tests declined from 10,763 to 7,806. This reduction in testing activity is a consequence of the previously mentioned change in testing practices among individuals receiving PrEP, who were previously tested regularly but are now tested only when symptomatic. The number of detected cases decreased from 1,269 in 2024 to 1,146 in 2025, with the largest decline observed in East Zealand and Jutland. North Zealand was the only province in which an increase in the number of cases of rectal chlamydia among males was observed from 2024 to 2025. At the national level, the positivity rate increased from 6.9% in 2024 to 8.0% in 2025, which may reflect the current strategy of more targeted testing of symptomatic individuals receiving PrEP.
Lymphogranuloma venereum (LGV)
At SSI, 1,467 samples were tested for LGV in 2025 using a nucleic acid amplification technique (NAAT). These samples originated from a total of 1,280 individuals, comprising 1,052 males, 222 females, and 6 individuals of unknown sex. This represents a decrease in the number of LGV tests performed compared with 2024, when 1,597 samples from 1,406 individuals were analysed. The largest decline in testing activity was observed among males, which may be attributable to the previously described testing strategy for individuals receiving PrEP. For both sexes, LGV testing was most commonly performed on anorectal samples, and in a small number of cases on pharyngeal or urogenital samples. A marked increase was observed in the number of samples in which a rectal swab was analysed together with a swab from another anatomical site, most often the pharynx. Alongside the decline in testing activity, the number of detected LGV cases decreased substantially from 140 positive samples corresponding to 135 episodes in 2024 to 82 positive samples corresponding to 78 episodes in 2025. An LGV episode is defined using the same temporal criteria as a chlamydia episode. Nationally, the number of LGV investigations decreased by 8%, while the number of detected LGV episodes decreased by 42% (from 135 in 2024 to 78 in 2025).
These findings are also described in EPI-NEWS 19–22b/2026.