No 20 - 2016
HAIBA 2015
Norovirus outbreak caused by lettuce
HAIBA 2015
2015 saw the establishment of national monitoring of three types of hospital-acquired infections through the Hospital-Acquired Infections Database (HAIBA), EPI-NEWS 9/15. HAIBA data go back as far as 2011. Before the introduction of HAIBA, these infections were monitored through prevalence studies that provided snapshots of the situation and which were performed only as cross-sectional checks at departments who participated voluntarily. With HAIBA it is now possible to follow the development of the selected indicators over time and for all hospitals and departments in Denmark.
In March 2015, HAIBA monitoring was launched for bacteraemia (bacteria in the blood) and intestinal infections caused by Clostridium difficile (C. difficile), and in October 2015 urinary tract infections were included, too. The results of the monitoring are published at eSundhed which is an interactive website that provides public access to health data. Furthermore, HAIBA can be accessed by following this link www.haiba.dk. Here, users can generate reports on the number and incidence of various types of infections per week or per month, and for any department/ward, hospital, region and for all of Denmark.
The objective of the HAIBA is to establish the basis for improvements of infection control. It is essential to note that HAIBA data reflect the clinical and diagnostic practice at the hospitals and the data will therefore be affected by any changes made, e.g. an increase in the diagnostic efforts, the introduction of novel diagnostic methods, changed guidelines, organisational changes and changes in coding practice. An increase or a decrease in incidence will therefore not always be straightforward to explain or interpret: In some cases, a real change in the incidence of infections may have occurred; in other cases, other explanations may apply. Through an active dialogue aiming at unearthing the trends, it will be possible to interpret HAIBA data locally and therefore to identify focus areas. Additionally, HAIBA serves to increase the attention given to infection hygiene, and studies show that an enhanced focus alone may contribute to a decrease in the occurrence of infections.
Background data
The HAIBA draws on data from the Danish Microbiology Database (MiBa) and from the National Patient Register (NPR). The information from these sources of data is combined and processed by use of algorithms with a view to identifying the various infections and to classify which infections are hospital-acquired. The algorithms were previously described in EPI-NEWS 10/15, 11/15 and 51/15. Additional details are available at the HAIBA website (www.haiba.dk) under “Documentation”.
In this issue of EPI-NEWS, we present the trends of the indicators selected for the 2011-2015 period. The presented figures, which show incidence by sex and age, are calculated on the basis of the underlying background data. For this purpose, all temporary civil register (CPR) numbers (with letters) have been removed. These CPR numbers comprise approx. 0.3% of all data, and the numbers therefore deviate marginally from the results presented at www.haiba.dk.
Developments in hospital-acquired bacteraemia
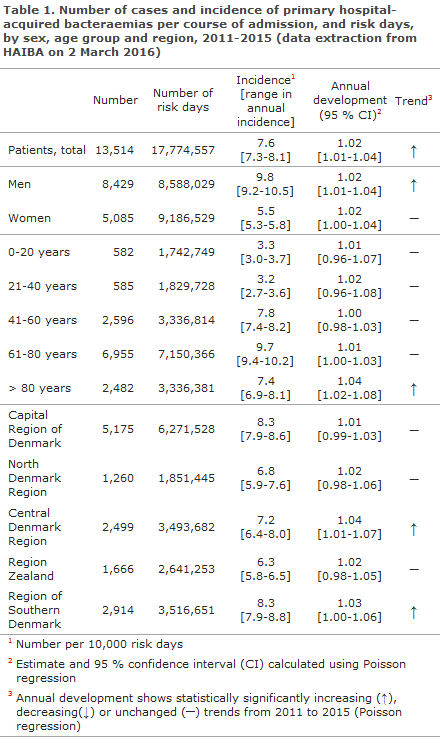
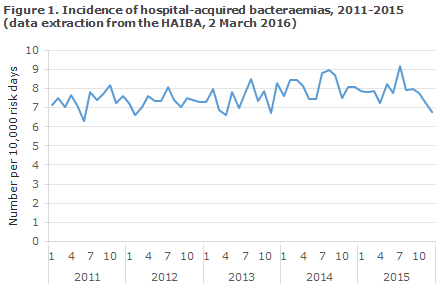
Bacteraemia, also known as blood poisoning, is a serious condition that is associated with a high mortality. The incidence of hospital-acquired bacteraemia was markedly higher among men than among women, and occurred more frequently in the older age groups, particularly in the 60-81-year age group, Table 1. The incidence of hospital-acquired bacteraemia followed an increasing trend throughout Denmark in the 2011-2015 period, Figure 1. Specifically, an increased incidence among men and in the 80+ year age group contributed to this increase. The incidence in the 60-81-year age group increased in the 2011-2014-period, but levelled out in 2015. Finally, there was considerable variation in the regional incidences, Table 1.
Developments in hospital-acquired urinary tract infection
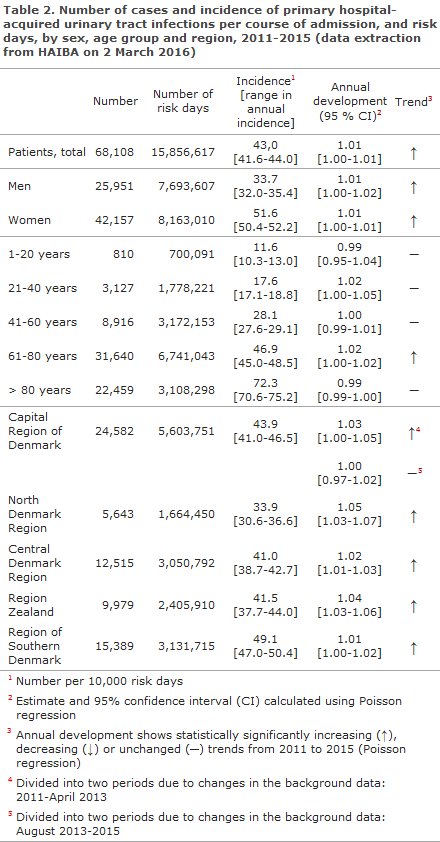
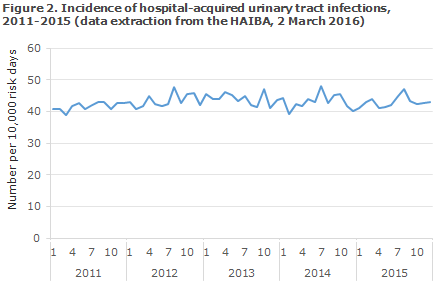
Urinary tract infection is a frequently occurring hospital-acquired infection that is mainly associated with use of urinary tract catheters and immobilisation. In HAIBA, children under one year of age are excluded from the algorithm on urinary tract infections as the sampling basis is different for this group of patients.
As expected, women (51.6 infections per 10,000 risk days) had a higher incidence than men did (33.7 infections per 10,000 risk days), and there was considerable difference between the age groups. A modest, but statistically significant increase in the incidence was seen in the 2011-2015 period, Figure 2. The increase was seen in the 61-80-year age group, among men and women alike. The increase over time was observed for all regions, but there were signs of a stabilisation in the Capital Region of Denmark in the final 2.5-year period.
Development in intestinal infections involving Clostridium difficile
C. difficile causes serious intestinal infections and is strongly associated with antibiotic treatment. As the bacterium produces spores capable of surviving in the environment, it can spread and cause outbreaks at hospitals. In 2008/2009, the Capital Region of Denmark was affected by several outbreaks, EPI-NEWS 13/09. It is likely that the infection subsequently spread to Region Zealand as patients were moved to this region, EPI-NEWS 7-8/12.
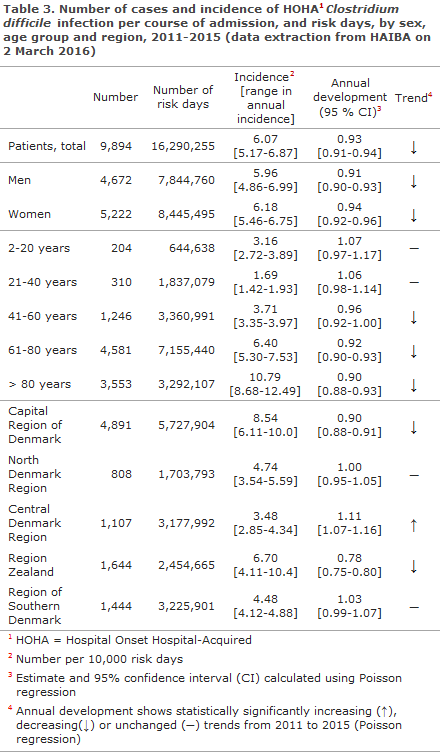
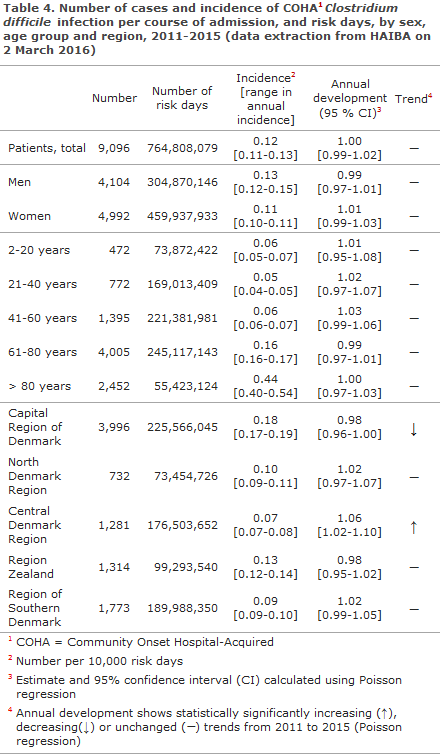
HAIBA presents figures on ’Hospital-onset Hospital Acquired’ C. difficile-infection (HOHA CDI) and ’Community-onset Hospital Acquired’ C. difficile infection (COHA CDI). Both types are related to admission or ambulatory treatment at hospitals: in HOHA, disease onset occurs during admission. In COHA, however, disease onset occurs after discharge, EPI-NEWS 10/15. Only figures on patients older than 2 years of age are included as it is uncertain if C. difficile may cause disease in the two first years of life.
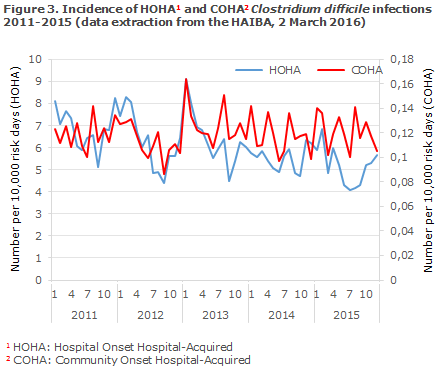
The incidence of COHA CDI, Table 3, and COHA CDI, Table 4, was higher among patients in the oldest age groups, and the highest incidences were seen in the Capital Region of Denmark and in Region Zealand. A clear decrease in the occurrence of HOHA was seen in the period, Figure 3. The decreasing trend was particularly marked in the Capital Region of Denmark (approx. 10 % annually) and in Region Zealand (approx. 22 % annually). Furthermore, the decreasing occurrence of HOHA was particularly pronounced in the older age groups, Table 3. Despite an increasing trend in the Central Denmark Region, the HOHA occurrence remained low in this region, Table 3.
Use of the HAIBA
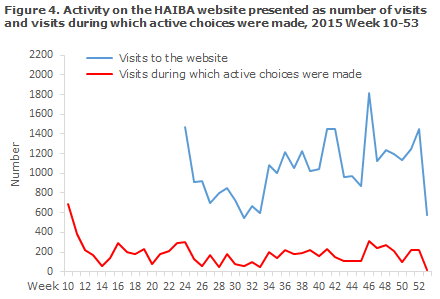
Since the launch of HAIBA, the number of visits during which the interactive section of the website is used has remained stable at around 180 weekly visits, Figure 4. The number of visits to the homepage was measured as from Week 24 2015 and increased from about 900 to 1,300 weekly visits (range 547-1,819 visits).
Additionally, several hospitals have enquired many times about possible explanations for the development in local numbers or to discuss how data may be used in practice to improve infection control. These contacts have been of great importance, both for the validation of HAIBA figures and to inform discussions about how to use HAIBA in practice.
Commentary
HAIBA, which has now been operational for one year, provides unique possibilities for ongoing monitoring of the development in hospital-acquired bacteraemia, urinary tract infections and C. difficile infections. It is our intention to expand HAIBA in the course of 2016 to include data also on selected post-operative infections.
A mentioned above, various factors may explain the trends seen over time, and it is important to keep this in mind when interpreting the data. For instance, some of the regional differences may be related to the composition of the patient population and regional diagnostic practices. For C. difficile, the known outbreaks and the handling of these outbreaks may explain both inter-regional differences and trends over time. In this issue of EPI-NEWS, we only describe some general trends.
The incidence of both hospital-acquired bacteraemias and urinary tract infections increased from 2011 to 2015, but only in a number of specific patient groups and in a limited number of regions. This may allow us to gain insight into the areas on which the infection control should focus. HAIBA records a nearly twice as high bacteraemia incidence for men as for women. Studies from other countries also describe that men are at a higher risk of developing bacteraemia, both hospital-acquired bacteraemia and bacteraemia in general. It is likely that a considerable share of these bacteraemias is caused of urinary tract infections as men have an increased risk that a urinary tract infection progresses into bacteraemia. Even though the incidence of hospital-acquired urinary tract infection is clearly higher among women than among men, urinary tract infections may have more serious consequences in men. This is also supported by the literature.
The high occurrence of C. difficile in the Capital Region of Denmark and in Region Zealand should be seen as a consequence of the outbreaks that occurred in these regions, including the special focus on diagnostics and monitoring as one of the precautions in connection with these outbreaks. It is very encouraging that the incidence is now decreasing in these regions, even in a situation in which more testing is performed than at the beginning of the period. For instance, as per 1 October 2015, Region Zealand has reorganised its diagnostic practice to introduce increased testing of elderly persons above 65 years and have therefore gained a 10% improvement with respect to diagnostics. Conversely, the incidence is increasing in the Central Denmark Region - even though it remains low here.
The observed increase may reflect that an additional spreading of C. difficile has occurred in Denmark, or that changes have occurred in the consumption of antibiotics. Nevertheless, the increase may also be artificial in the sense that it may reflect improved diagnostics and increased attention. It is not currently possible to use HAIBA to differentiate between the involved C. difficile types, e.g. between the serious CD027 type and other highly virulent types. It is therefore desirable to investigate the trends in more detail, and to study diagnostic practices and the transmission dynamics of the various types in order to contribute to curbing any spreading to the extent possible. In EPI-NEWS 10/15, HAIBA showed an increase in COHA incidence, but that increase was due to an error that occurred in connection with an amendment of the algorithm.
Hospitals have started considering how HAIBA may be used optimally. Aggregated data are mostly useful for analysis of trends as illustrated in this annual report. Locally, stakeholders may analyse their own figures in much the same way and assess trends. But comparison of departments, hospitals or regions is an entirely different matter as a range of factors affect the results making them unfit for comparisons. These factors include underlying diseases, MiBa and NPR coding practices and culture practices. It may be useful to assess these differences and thereby elucidate the differences with respect to background data, patient groups and distribution of infections. But the observed differences cannot be employed directly to identify departments, hospitals or regions in which the risk of infection is high.
It should also be mentioned that HAIBA is a dynamic system based on data sources that are regularly being updated and validated, and this means that the data basis is also changing. For instance, information in the NPR is continuously being updated and validated and this causes the data basis to change. The wording and design of the results provided by the departments of clinical microbiology also change over time, which triggers a need for adaptation in HAIBA. Scientific studies may also produce novel knowledge which, in turn, gives rise to adjustment of case definitions.
Additionally, the healthcare system is changing rapidly towards shorter admission periods and more prolonged ambulatory courses. This means that the traditional divide between hospital-acquired and community-acquired infections is disappearing. HAIBA needs to harbour these changes and to be adapted to accommodate them. For instance, it may be considered in the future if incidence based on days at-risk is still relevant of if the starting point should rather be specific exposures. For these reasons, HAIBA figures may change over time both prospectively and retrospectively because of re-calculation of reports from previous years.
The hospitals have voiced a request for further development of HAIBA to strengthen the use of data and to improve the opportunities for applying the data in practice. If, e.g., the hygiene organisations were given access to patient-specific data flagged by HAIBA, their chance of using HAIBA would be strengthened considerably. Steps are being taken to provide a solution in this area that is both legally and technically viable. Additionally, there is a wish to include more new types of infections to be able to give relevant indicators for more fields. In the course of 2016, we expect to add infections that occur following the insertion of hip and knee prostheses. Efforts are also being made to provide a technical solution that sends aggregated data to the regions which will allow the hospitals to automatically prepare reports based on HAIBA data.
After the first year in which hospitals, regions and Statens Serum Institut gained their initial experiences with the use of HAIBA, we hope that HAIBA will become even more integrated into the daily work with infection hygiene in 2016. Furthermore, indicators from the HAIBA will form part of the New Danish Quality Programme.
(S. Gubbels, J. Nielsen, M. Voldstedlund, M. Chaine, K. Mølbak, Department of Infectious Disease Epidemiology, B. Kristensen, Central Unit for Infectious Hygiene, Statens Serum Institut, K. S. Nielsen, Danish Health Data Authority, H.C. Schønheyder, Department of Clinical Microbiology, Clinical Diagnostics, Aalborg University Hospital, J.K. Møller, Department of Clinical Microbiology, Hospital Lillebælt, Vejle Hospital, B. Lundgren, Centre of Diagnostic Investigation, Rigshospitalet, J. Utzon, Centre for Health, Unit for Quality and Patient Safety, Capital Region of Denmark, J. Engberg, Department of Clinical Microbiology, Slagelse Hospital, P.D. Cramon, Region Zealand, S. Ellermann-Eriksen, Department of Clinical Microbiology, Aarhus University Hospital, E. Lyngsø, Corporate Quality, Regionshuset Viborg, Central Denmark Region, A. Holm, Department of Clinical Microbiology, Odense University Hospital, J. Kjær-Rasmussen, Healthcare Planning, Patient Dialogue and Quality, North Denmark Region)
Norovirus outbreak caused by lettuce
In the first week of April 2016, several outbreaks with gastro-intestinal infections were reported, and Food Control Office Zealand/Funen quickly suspected the coral lettuce Lollo Bionda as a joint cause of infection. The Danish Veterinary and Food Administration in collaboration with Statens Serum Institut and the Technical University of Denmark (DTU) initiated a comprehensive investigation to establish if the outbreaks were related, which agent had caused the illness and if the lettuce was, indeed, the common source of infection for all of the observed outbreaks.
A total of 23 outbreaks were investigated, including 1,497 persons from various companies, e.g. course attendants and restaurant visitors. Among these, 412 (28%) persons fell ill with vomiting and/or diarrhoea. Epidemiological cohort studies performed in two of the affected companies pointed towards dishes that included the Lollo Bionda lettuce. This was underpinned by investigations from other companies that had all received the same lettuce. Tracking of the lettuce from the various outbreaks demonstrated that the product in question was a Lollo Bionda lettuce of French origin marketed by a single company. The product was primarily sold to restaurants and catering companies through a wholesale merchant, who on 7 April volunteered to withdraw the salad.
Symptoms pointed towards a norovirus infection which was confirmed on the basis of 28 patient samples in which norovirus of genogroup I (GI) was found. Additional typing of virus from 22 patients from a total of nine different companies demonstrated that all had the same subtype of norovirus (genotype GI.P2-GI.2), which supported the hypothesis of a common food-borne source of infection. To secure faeces samples for testing, the Danish Veterinary and Food Administration and Statens Serum Institut handed out specimen containers and pre-paid response envelopes directly to any diseased persons at the affected companies. The samples were sent to Statens Serum Institut where they were subsequently tested for both virus and bacteria, and were subtyped so that samples from different regions could be compared and linked. Concurrently, DTU Food tested lettuce from several outbreaks, and in one head of lettuce the Institute found a low number of norovirus of the same genogroup found in the patients.
Commentary
The cause of the contamination of the lettuce remains unknown. This is the second time that Lollo Bionda lettuce from France has caused a series of outbreaks - the first time was in 2010 (EPI-NEWS 5/10). This is the first time that a norovirus outbreak in Denmark has provided such large number of human samples from various sub-clusters during the investigation. The proactive handing-out of specimen tubes from first contact and the national-level collection of the samples for testing for a broad spectrum of agents and for subtyping were instrumental in understanding the big pig picture in time and also in facilitating the linking of patients across various focal outbreaks. The outbreak demonstrates that contaminated lettuce sold to catering companies holds a considerable potential for infection of a large number of persons within a very limited time span which, in turn, underlines the importance of rapid investigation, timely sampling of patients and foods, and of willingness to withdraw products on the part of the foodstuffs companies based only on a suspicion with respect to the source of infection.
(L. Müller, K. Mølbak, Department of Infectious Disease Epidemiology, L.D. Rasmussen, Department of Microbiological Diagnostics and Virology, T. Jensen, Danish Veterinary and Food Administration, A.C. Schultz, DTU Food)
Link to previous issues of EPI-NEWS
18 May 2016