No 48 - 2013
Hepatitis A 2012
Major hepatitis A outbreak caused by frozen strawberries
Hepatitis A vaccines from the SSI
World AIDS Day 1 December
Form 1510 can no longer be ordered from Dafolo
Hepatitis A 2012
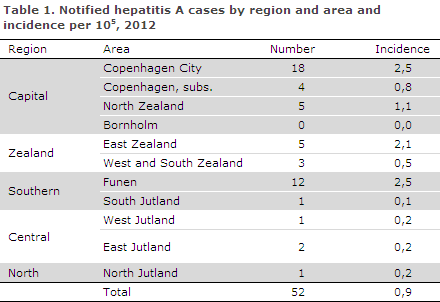
2012 saw a total of 52 cases of hepatitis A virus (HAV) infection in Denmark, including 29 women and 23 men. The number of notified cases and the incidence per 105 persons by administrative region and area are presented in Table 1.
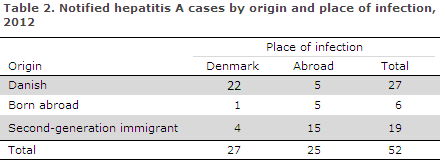
Notified cases by origin and place of infection are presented in Table 2.
Infection abroad
Five Danes were probably infected abroad; in Pakistan, Egypt, Italy and Turkey, whereas the country of infection remained unknown for one case. Among five cases born and infected abroad, three were infected before arriving to Denmark; in the Philippines (2) and India (1). Furthermore, one case was infected during a family visit to Pakistan. The final case was infected during a tourist or business trip to Egypt. A total of 15 second-generation immigrants were infected abroad, all in connection with family visits in the following countries: Pakistan (7), Iraq (3), Kenya (3), Morocco (1) and Somalia (1).
Infection in Denmark
A total of 27 notified cases were probably infected in Denmark. Among these, 17 (63%) were possibly associated with food-borne outbreaks (see the below section for details). In the remaining ten cases, the source of infection was stated as infection from a member of the household (4), from a child in a day-care institution (1), drug addict risk behaviour (1), via food (1) and unknown (3).
Outbreaks
In 2012, three HAV outbreaks were investigated in which the presumed source of infection was foods sold in Denmark.
Outbreak I: In January-February 2012, six persons, including three children below 15 years of age, tested HAV positive; all of these were genotype 1B cases. The virus RNA sequence was identical in the six persons, which strongly indicates that they had been subject to the same source of infection. On the basis of interviews with the patients, it was not possible to establish a specific food item as the vehicle of infection.
Outbreak II: In November-December 2012, a cluster of six cases was reported in the Odense area. Virological testing confirmed the suspicion of an outbreak as virus RNA sequencing detected identical genotypes (1B). On the basis of interviews and the fact that the cases fell ill within the same short time span, the outbreak seems to have been locally confined and possibly food-borne. It was, however, not possible to establish the source of infection.
Outbreak III: In December 2012, another six HAV genotype 1B cases were reported; phylogenetic comparison of these cases showed a greater similarity with European HAV genotype 1B cases than with the previously established Danish genotype 1B cases. This proved to be the beginning of a large international genotype 1B outbreak which was to continue into 2013. In this outbreak, the source of infection was identified as frozen strawberries (see a detailed description later in this issue of EPI-NEWS).
Development in hepatitis A, 1990-2012
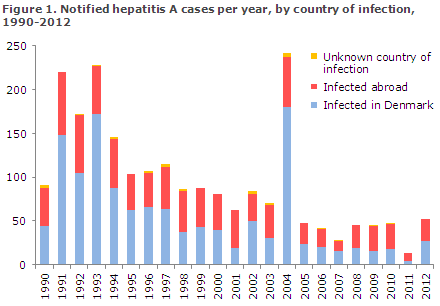
The number of notified HAV cases from the 1990-2012 period is presented in Figure 1. Since the mid-1990s, the number of notified cases has decreased, except for 2004 which was characterised by a major outbreak among men who have sex with men, EPI-NEWS 52/04. The share of persons infected in Denmark has also decreased during the period.
Virus typing
Routine HAV typing has been performed since 2006. Thus, positive HAV IgM serum specimens are sent to the Section for Virology Surveillance and Research, Statens Serum Institut to characterise the specimens through PCR typing and sequencing. In 2012, a total of 27 specimens from notified cases tested positive for HAV along with an additional six specimens from non-notified cases. Typing was possible in 27 of the 33 (82%) specimens.
The typing results showed that 20 cases (74%) were genotype 1B, six cases (22%) were 3A and a single case (4%) was genotype 1A. The cases forming part of Danish outbreaks were all genotype 1B (14 cases), and an additional two cases were infected with genotype 1B in Denmark with no known association with an outbreak, whereas four genotype 1B cases were infected abroad (Kenya, Egypt, Thailand and Iraq). A travel history was known for five of the six genotype 3A cases, including two cases who were infected in Pakistan, one in Egypt and two in Denmark. The genotype 1A case had visited Turkey.
Commentary
In 2012, the number of cases notified with acute hepatitis A was in line with previous years, apart from 2011 when the number of notified cases was lower than in the other years, EPI-NEWS 49/12. Approximately half of the notified cases were infected in Denmark. This was primarily due to three outbreaks of which one marked the beginning of a major international food outbreak in 2013 (see below).
HAV has a considerable outbreak potential in susceptible populations such as the Danish population; and increasing international trade in fresh and frozen foods, including fruit and vegetables from HAV endemic countries, increases the risk of infection via ingestion of HAV contaminated foods. Outbreaks caused by imported berries, fruit and vegetables are a growing problem which was previously seen for e.g. norovirus, EPI-NEWS 05/11 and Shigella sonnei, EPI-NEWS 36/09.
This underlines the importance of timely reporting of all HAV cases and of having the specimens genotyped and analysed. Typing through sequencing makes it possible to quickly discover outbreaks, to differentiate between imported and non-imported cases in an attempt to establish the country of origin and the food item responsible for the outbreak, and to identify any sources of infection to prevent further disease.
As previously, a considerable share of those who are infected abroad are children of immigrants infected during visits to their parents' country of origin. It is important to provide advice on hepatitis A vaccination for this group.
(L. Müller, S. Ethelberg, S. Cowan, Department of Infectious Disease Epidemiology, H. Vestergaard, T.K. Fischer, S. Midgley, Microbiological Diagnostics and Virology)
Major hepatitis A outbreak caused by frozen strawberries
On the basis of an increase in the number of notifications, Statens Serum Institut (SSI) initiated an investigation into a hepatitis A virus (HAV) outbreak in February 2013. The patients who had had no travel activity within 2-6 weeks before symptom onset did not belong to the traditional hepatitis A risk groups and lived at various locations scattered across Denmark.
Furthermore, HAV typing from these patients showed that several patients had been infected with the same genotype 1B and that several had the same sequence, which indicated a shared source of infection. Introductory interviews showed that the patients had no immediate contact to each other, and that it was probably a national food-borne HAV outbreak.
On the basis of the introductory interviews, the SSI initiated a case-control study to identify the source of infection. As part of the study, the patients' answers to a series of questions inviting them to detail it they had ingested a range of specific food items were compared with the answers from a comparable group of healthy Danes.
The study indicated that the source of infection was probably frozen berries, particularly frozen strawberries that had been ingested without previous heat treatment, e.g. in desserts or smoothies. This finding was made public on 14 March 2013. On the same day, the Danish Veterinary and Food Administration introduced a recommendation that all types of frozen berries should be parboiled for at least one minute before being used in smoothies, cake toppings or desserts.
On 1 March 2013 and through the ECDC (European Centre for Disease Prevention and Control), the SSI informed the other European countries of the presumed food-borne outbreak. Finland, Norway and Sweden reported that they had also received an increased number of hepatitis A notifications in cases with no previous foreign travel activity.
A comparison of HAV sequences showed that several of the cases in the three other countries had the same genotype and sequence as the Danish cases. It was thus established that it was a single Nordic outbreak. The three remaining countries also conducted case-control studies and a combined analysis for all four countries indicated that the source of the outbreak was frozen strawberries.
The food authorities analysed the distribution of frozen berries, particularly frozen strawberries to the four countries, and undertook reverse tracking of frozen berries based on specific information from a number of patients. The analyses indicated that frozen strawberries of Egyptian or Moroccan origin harvested in 2012 and packaged by a Belgian company were the source of the outbreak. However, it has not been possible to determine with certainty the origin of the berries. Direct detection of HAV in food items, including frozen strawberries, was not possible.
As a consequence of the epidemiological results and the food authorities' analyses, COOP in Denmark, Norway and Sweden on 30 May 2013 effected a voluntary recall of all frozen strawberries from Egypt and Morocco which they had received from their Belgian supplier.
The outbreak was declared to have concluded 15 October 2013. Only three cases forming part of the outbreak were recorded in Denmark as from 1 July 2013; symptom onset of the last case occurred on 8 August 2013.
Outbreak overview
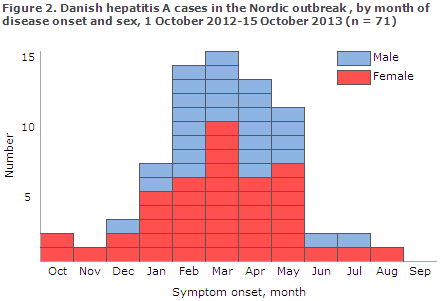
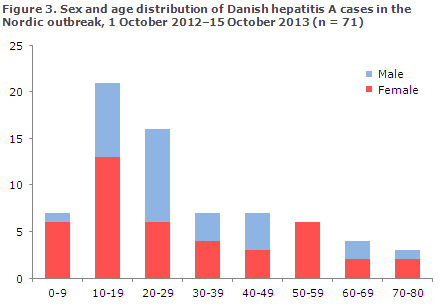
In the period from 1 October 2013 to 15 October 2013, Statens Serum Institut has recorded 71 hepatitis A cases belonging to the outbreak, Figure 2. Of these, 42 (59%) were women and 29 (41%) were men. The youngest case was two years old and the oldest 80 years old. However, the majority of cases (52%) were 10-29 years old, Figure 3. The cases resided in various locations across Denmark. Of the 71 Danish cases, seven were in all probability due to person-to-person transmission.
In all, the four Nordic countries recorded 114 cases belonging to the outbreak. The cases included 70 (61%) women, and 55 (48%) of the cases occurred in persons aged 10-29 years.
Commentary
The described outbreak is the first general food-borne hepatitis A outbreak in Denmark. The outbreak was identified through the national, clinical surveillance system which underlines that the importance of doctors examining patients with relevant HAV symptoms, even if these have no travel history, and that the cases are reported timely.
Furthermore, the existence of seven cases who were infected through person-to-person transmission underlines the importance that doctors contact the Regional Medical Officers of Health with no undue delay to assess the opportunity of post-exposure vaccination of close contacts. Ideally, this should happen immediately after the index patient presents his complaint to the doctor or as soon as the laboratory diagnosis is available.
Food-borne hepatitis A outbreaks caused by frozen berries have previously been seen, among others in North America. Furthermore, this year frozen berries were established to be the source of infection in concurrent hepatitis A outbreaks in the USA, Italy and Ireland. It should be noted that this occurred in the wake of the Danish and subsequent Nordic study.
It should also be noted that in relation to the Italian outbreak, investigators managed to detect virus from berries, which is a technically complicated task. The outbreaks give rise to consideration as to whether frozen berries may also be the source of infection in sporadic HAV cases for which no other probable exposures exist.
An important element of outbreak identification and investigation was associated with the opportunity to perform HAV typing on material from patients, as this made it possible to confirm the outbreak, initially in Denmark and subsequently in the three other Nordic countries. Typing has also allowed us to show that the HAV types of the Nordic outbreak were different from the types of the concurrent HAV outbreaks occurring in other countries.
In Denmark, the outbreak was investigated through the cooperative efforts of Statens Serum Institut, the Danish Veterinary and Food Administration and the Danish Food Institute under the auspices of The Central Outbreak Management Group.
The SSI published the first news article on the outbreak on 3 March 2013, and has previously informed of the outbreak in EPI-NEWS 22/13.
(S. Gillesberg Lassen, S. Ethelberg, K. Mølbak, Department of Infectious Disease Epidemiology, T.K. Fischer, A. Hintzmann, S. Midgley, Department of Microbiological Diagnostics and Virology)
Hepatitis A vaccines from the SSI
Statens Serum Institut has put out a tender on hepatitis vaccines and will in future supply the hepatitis A vaccine Epaxal® when hepatitis A vaccines are ordered for children as well as adults. Until mid-January, both Havrix® and Epaxal® will be supplied until exhaustion of all pack sizes of the Havrix® stock. Prices and pack sizes are available at the SSI's website.
Epaxal® contains no aluminium, but apart from that it is comparable to Havrix®. The vaccine is indicated for protection against hepatitis A in children over 1 year of age and in adults. The dose is 0.5 ml given intramuscularly in the deltoid region. In patients with reduced clottability, the vaccine may be administered subcutaneously in the upper arm.
To ensure long-term protection, a booster dose is to be given 6-12 months later. Based on limited experiences from healthy adult travellers, the booster may be given until 10 years after the initial vaccination. Based on a mathematical model and extrapolation from antibody decay, the protective effect will endure for a minimum of 30 years in a minimum of 95% of all fully vaccinated persons.
Epaxal® can be used interchangeably with other inactivated hepatitis A vaccines as the first and second (booster) dose. The vaccine contains remnants of egg protein and is contra-indicated in persons with known hypersensitivity to egg, chicken protein or formaldehyde. Furthermore, the vaccine may contain traces of polymyxin B.
Epaxal® should be administered with caution in breast-feeding women. For information on vaccination of pregnant women, please see EPI-NEWS 26a/13. The most frequently reported adverse reactions are mild and short lasting. These include fatigue (6-32%), pain at the injection site (5-25%) and headache (6-25%). For further information, please refer to the summary of product characteristics.
(B. Neale, Sales and Marketing, P.H. Andersen, Department of Infectious Disease Epidemiology)
World AIDS Day 1 December
The objective of World AIDS Day is to create awareness of the global as well as local fight against HIV and AIDS.
In Denmark, the main problems of HIV prevention is that far too many HIV positives are tested late in their disease course, and that the disease is shrouded in discrimination and stigma, not least due to ignorance.
On this basis, this year will see the introduction of campaigns to increase awareness of the need for timely testing, www.hivtestingweek.eu, and campaigns to reduce ignorance and prejudice, www.aidsfondet.dk.
At the SSI's website, the World AIDS Day is marked by the publication of a news article (LINK).
(Department of Infectious Disease Epidemiology)
Form 1510 can no longer be ordered from Dafolo
Syphilis and gonorrhoea are notified to the Department of Infectious Disease Epidemiology on Form 1510s and Form 1510g, respectively. The forms are available for download from www.ssi.dk (Health data and ICT/Surveillance in Denmark/Mandatory notification systems). Until now, it has been possible for doctors to order the green common form used for syphilis and gonorrhoea from Dafolo, but that is no longer possible.
(Department of Infectious Disease Epidemiology)
Link to previous issues of EPI-NEWS
27 November 2013