No 26 - 2026
Dermatophilosis – new European cases suggest human-to-human transmission /
Methicillin-resistant Staphylococcus aureus (MRSA), 2025
Dermatophilosis – new European cases suggest human-to-human transmission
Dermatophilosis is a rare bacterial skin infection caused by Dermatophilus congolensis. The infection occurs primarily in livestock and wild animals and has traditionally been regarded as a rare zoonosis, with humans becoming infected through contact with infected animals or contaminated environments.
However, during 2025-2026, several cases have been reported from France, Germany, Spain, and Sweden, suggesting that transmission has occurred between humans. Most cases have been described among men who have sex with men (MSM), and preliminary investigations indicate that close skin-to-skin contact, including sexual contact, is likely to be the principal route of transmission. Several cases reported prior attendance at so-called sex-on-premises venues, including saunas, where close physical contact may occur.
In addition, cases were reported in Norway in 2025 among individuals practicing martial arts, suggesting that transmission may also occur through other forms of close physical contact. Transmission via contaminated environments or fomites cannot be excluded.
Clinical presentation
The infection is generally mild. Dermatophilosis typically presents with papules, pustules, scaly skin lesions, or crusted skin lesions. The lesions may be pruritic, and folliculitis may occur. Systemic symptoms are rare.
In the recently reported European cases, the lesions have been located predominantly in the genital area, on the face, chest, and extremities. The incubation period is not well characterized, but in the French cases the median incubation period was estimated to be approximately six days. The reported cases have generally followed an uncomplicated clinical course, with no hospitalizations or serious complications.
Diagnostics
The diagnosis is established by microbiological examination of specimens obtained from skin lesions. D. congolensis can be cultured from lesions and identified by MALDI-TOF or molecular methods, including 16S rDNA analysis.
Treatment
Dermatophilosis may be self-limiting, but antibiotic treatment is recommended for confirmed cases, among other reasons to shorten the duration of illness and potentially reduce onward transmission. Treatment may include β-lactam antibiotics or macrolides, as well as topical antibiotic therapy. The European cases reported to date have all had a mild and uncomplicated clinical course and have responded well to treatment.
Assessment of the situation
SSI supports the European Centre for Disease Prevention and Control (ECDC) assessment that the risk of transmission in the general population is very low. Among men who have sex with men (MSM) with multiple sexual partners, the risk is considered low, while the likelihood of transmission is considered moderate among MSM with multiple sexual partners who visit sex-on-premises venues. However, the overall risk for this group is still considered low, as the disease has so far followed a mild clinical course.
There are still substantial uncertainties regarding the routes of transmission, incubation period, duration of infectiousness, and the true extent of spread, as the infection is rare in humans and may be underdiagnosed.
Recommendations
Although dermatophilosis remains a rare human infection, clinicians and Departments of Clinical Microbiology (DCMs) should be aware of the disease in patients presenting with compatible skin lesions, particularly when there is a history of relevant exposure.
Patients with suspected or confirmed dermatophilosis should avoid close skin-to-skin contact, including sexual contact, until their skin lesions have healed. They should also avoid sharing towels, clothing, and bed linen and maintain good hand and personal hygiene. Condoms do not in themselves protect against transmission of D. congolensis, as infection may occur through direct contact with affected skin.
Notification
Dermatophilosis is not a notifiable disease in Denmark. However, because human dermatophilosis remains a rarely reported disease and cases of newly recognized human-to-human transmission have now been reported, suspected outbreaks or clusters of cases should be notified under List 1A, regardless of whether the cause is known or unknown. See the guidance on notification of diseases listed under List 1A.
Further information is available in SSI's Disease Lexicon entry on dermatophilosis.
(K. Bray, M. Wessman, Department of Infectious Disease Epidemiology and Prevention, A. Ronayne, J. Skov Jensen, Bacteria, Parasites and Fungi)
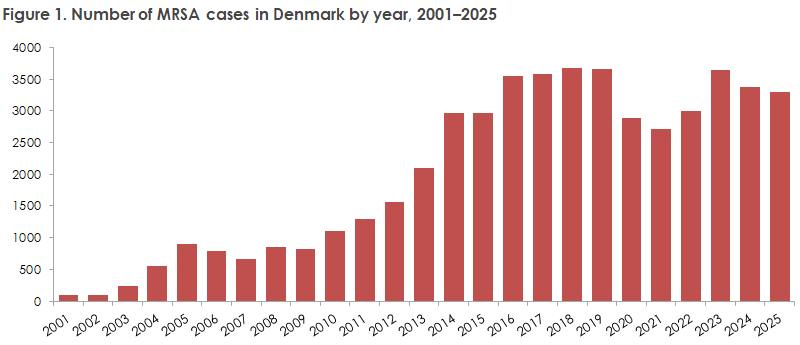
Methicillin-resistant Staphylococcus aureus (MRSA), 2025
The number of new MRSA cases was 3,301 in 2025 (Figure 1), which was at the same level as in 2024 (3,372), see EPI-NEWS 43b/2025. 58% of cases presented with symptomatic infections, the majority of which (80%) were skin and soft tissue infections.
There were 66 cases of Staphylococcus aureus bacteremia (SAB) caused by MRSA in 2025, accounting for 2.8% of all SAB cases. This is the highest proportion recorded in the past 20 years but remains low in an international context.
For a detailed epidemiological description of the occurrence of MRSA in 2025, please refer to the Annual Report on MRSA 2025.
In 2025, a total of 36 MRSA outbreaks were recorded in hospitals, nursing homes, and other institutions. These involved 118 cases, including 56 with infection and 62 identified through screening and contact tracing. Most outbreaks involved one to five patients. The largest outbreak involved 18 patients and originated in a neonatal unit. Of the 36 outbreaks, seven occurred in neonatal units. In addition, there were 15 outbreaks in nursing homes and associated with home-care services (39 patients in total) and 10 outbreaks in hospital departments other than neonatal units (24 patients).
Despite these outbreaks in healthcare settings, the risk of acquiring MRSA in Danish hospitals remains low.
The number of cases caused by livestock-associated MRSA CC398 was 591, accounting for 18% of all new cases, the lowest proportion since 2012 (15%). In 2025, 91 individuals without livestock contact developed infections with livestock-associated MRSA CC398. This is comparable to previous years, indicating that the spread of livestock-associated MRSA CC398 in the general population does not appear to be increasing.
In 525 cases (16%), MRSA was acquired abroad, representing a typical proportion of cases.
There were 1,074 community-acquired MRSA infections, accounting for the largest share of all MRSA infections (55%).
(A. Petersen, A.R. Larsen, Bacteria, Parasites and Fungi, T. Urth, Department of Infectious Disease Epidemiology and Prevention)