No 5 - 2025
The season for free RSV vaccination for pregnant women ends on 31 January – the programme will resume on 1 May 2026 /
Tuberculosis in 2024 /
Atypical/nontuberculous mycobacteria (tuberculosis-like bacteria)
The season for free RSV vaccination for pregnant women ends on 31 January – the programme will resume on 1 May 2026
On 1 October 2025, the vaccination programme for pregnant women against RSV came into effect with the aim of protecting newborn children against severe RSV disease during the first months of life.
There has been strong support for the programme among both healthcare professionals and pregnant women. Figures from Statens Serum Institut show that as of 27 January 2026, 24,604 women had been identified who were assessed to have been in weeks 30–36 of pregnancy since 1 October 2025. Among these women, uptake of the RSV vaccination programme is 67%.
For information, the current season’s offer of free vaccination against RSV for pregnant women ends on 31 January 2026. The programme will start again on 1 May 2026. This means that pregnant women who reach week 32 during February, March and April, and who therefore have due dates in April, May and June respectively, are not covered by the vaccination programme. This is because RSV infection primarily occurs during the autumn and winter months, and children born in late spring and early summer are therefore not expected to be born into the RSV season.
Current knowledge about the effect and duration of the RSV vaccine also shows that the vaccine protects the infant during the first months after birth. Therefore, vaccination is only offered to pregnant women if their child will be at risk of severe RSV disease during the first vulnerable months of life. Accordingly, vaccination is only recommended in the period from May up to and including January, corresponding to pregnant women with due dates from July up to and including March. The Danish Health Authority recommends that pregnant women be vaccinated against RSV in each new pregnancy if the pregnant woman has a due date from July up to and including March.
Further detailed material about the vaccination offers for pregnant women, including information sheets with answers to frequently asked questions, can be accessed on the Danish Health Authority’s materials page and will be updated on an ongoing basis. The page also contains citizen-oriented material for printing, which has been translated into various languages, such as Arabic, Turkish and Urdu.
(The Danish Health Authority)
Tuberculosis in 2024
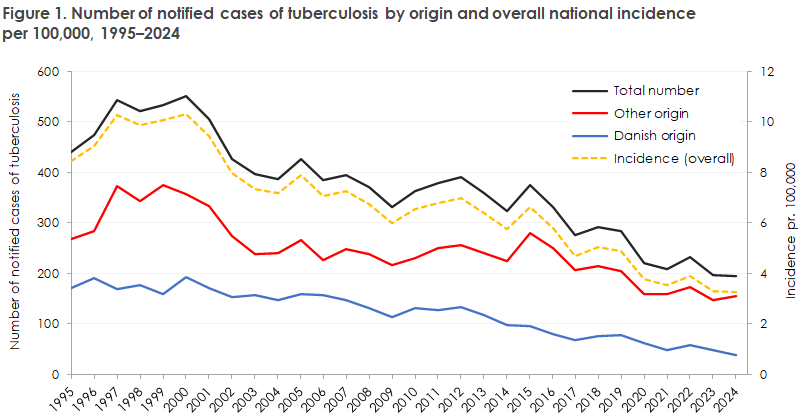
Tuberculosis (TB) is a relatively rare disease in Denmark. In 2024, 194 cases of the disease were identified, corresponding to an incidence (number of new annual cases relative to the population size) of 3.3 per 100,000. Denmark is therefore a so-called low-incidence country in the WHO context, whereas countries such as South Africa and India, with incidences in 2024 of 389 and 187 per 100,000 respectively, are high-incidence countries.
For a detailed epidemiological description of the occurrence in 2024, reference is made to Tuberculosis – summary of disease occurrence in 2024.
The occurrence of TB in Denmark has, with minor fluctuations, declined steadily over the past 25 years from 10.3 cases per 100,000 in 2000 to 3.3 per 100,000 in 2024, Figure 1.
Geographically, the incidence of TB is highest in the Capital Region of Denmark (4.5 per 100,000) and lowest in Region Zealand (1.9 per 100,000). This distribution has remained unchanged over a number of years.
The incidence of TB depends on country of origin. A total of 39 (20%) of TB cases in 2024 occurred among persons of Danish origin, corresponding to an incidence of 0.8 per 100,000, while 155 cases occurred among persons of origin other than Danish, corresponding to an incidence of 16.4 per 100,000. Within the latter group, there are also substantial differences, with the highest incidences seen among persons with ties to Greenland, Eritrea, Somalia, the Philippines, and Pakistan. The highest incidence is seen among persons of Greenlandic origin, where the incidence has remained consistently high over a number of years. This was described in a scientific article in 2025.
Nearly half (44%) of those infected were reported as having been infected in Denmark, 51% abroad, while the place of infection was unknown for 5%. This distribution has remained unchanged over the past 10 years. The fact that 44% were presumed to have been infected in Denmark, and that this has remained unchanged for many years, shows that there is still a great need to identify and break chains of transmission in Denmark.
The age distribution of TB also depends on country of origin. Among persons with TB of Danish origin, the median age was 56 years in 2024, unchanged from 2023. For persons of origin other than Danish, the median age was 36 years, representing a decrease from 2023 (43 years). There are also differences in the age profile of TB cases between the two groups, with the highest incidence among persons of Danish origin occurring in the 50–69-year age group, while the highest incidence among persons of origin other than Danish occurred in the 20–49-year age group. This difference has remained unchanged over the past 10 years.
The localization of TB also differs between persons of Danish origin and persons of origin other than Danish. Among persons of Danish origin, 90% have pulmonary TB, while among persons of origin other than Danish, pulmonary TB accounts for 60%. This distribution has been stable over a number of years.
A total of 16 TB cases were reported among children under 18 years of age in 2024. This was slightly more than in previous years (eight in 2022, 12 in 2023). Nine were born in Denmark, of whom four were infected in Denmark and five abroad. Eight of the Danish-born children were born to parents with ties to another country, and one child was born to Danish parents. Of the seven children born abroad, six were reported as having been infected abroad and one in Denmark. Although the number of children and adolescents reported with TB remains relatively low, approximately one third of the reported cases in 2024 were infected in Denmark. This means that continued attention to contact tracing in Denmark is necessary.
In summary, the 2024 data show that the incidence of TB continues to decline, with an unchanged distribution of cases by sex, age, origin, and disease manifestation over the past 10 years.
However, the disease has not been eliminated, especially not in risk groups, where substantial transmission and delayed diagnosis are still observed. It therefore remains important to conduct active screening in risk groups and systematic contact tracing for all new TB cases. To ensure accurate data, all TB cases must be reported; this is particularly important for cases diagnosed solely on the basis of clinical criteria.
(L.H. Holm, A. Koch, Department of Infectious Disease Epidemiology and Prevention, T. Lillebæk, D.B. Folkvardsen, H.J.N. Lorentsson, Department of Tuberculosis and Mycobacteria)
Atypical/nontuberculous mycobacteria (tuberculosis-like bacteria)
Mycobacteria that do not cause tuberculosis (TB) or leprosy are referred to as atypical or nontuberculous mycobacteria (NTM). This is a heterogeneous group of more than 200 different bacterial species that are widespread in the environment. Only a small proportion of these species cause disease in humans.
In Denmark as well as globally, an increasing incidence of disease caused by NTM is being reported. The increase is attributed to a combination of increased life expectancy, chronic—especially structural—lung disease, and more widespread use of immunosuppressive medications, all of which increase the risk of disease caused by these low-virulence bacteria.
In Denmark, approximately 100–150 cases of NTM disease are seen annually, of which about three quarters consist of pulmonary infections, followed by infections of lymph nodes, skin, and soft tissues. In rare cases, disseminated infection is seen, almost exclusively in immunosuppressed patients. It is important to emphasize that NTM—unlike TB—are not transmitted from person to person.
Due to the increasing incidence of especially NTM pulmonary disease, it is important to be aware of this diagnosis. Risk factors and symptoms that should raise suspicion include existing lung disease, especially bronchiectasis, COPD, asthma, cystic fibrosis, previous TB, other structural lung disease, and pectus excavatum. Characteristic symptoms include weight loss, night sweats, fatigue, cough (possibly productive), hemoptysis, dyspnea, poor response to empirical antibiotics, and radiological changes on chest imaging.
In extrapulmonary NTM disease, swollen lymph nodes or skin and soft tissue infections such as nodules, abscesses, cellulitis, or pustules are typically seen, often localized to the extremities. More rarely, deeper soft tissue infections, ulcerated nodules, or bullae occur. Lesions are most often solitary but may be multifocal, especially in immunocompromised patients.
In infections that do not respond to standard antibiotic treatment, NTM disease should be considered, particularly if histological examination reveals necrotizing or non-necrotizing granulomatous inflammation.
Most NTM species can be diagnosed as part of standard testing for mycobacteria performed at Statens Serum Institut. A positive finding must be interpreted with caution, and repeated samples may be necessary, as there is a risk of both false-positive findings (contamination or colonization) and false-negative results.
Diagnosis and treatment of NTM are specialist tasks and are most often managed by pulmonary medicine, infectious diseases, and pediatric departments in collaboration with the Department of Tuberculosis and Mycobacteria at Statens Serum Institut. Any treatment always consists of prolonged (months to years) multidrug antibiotic therapy, several of which have potentially serious side effects. Treatment modifications are therefore often necessary. NTM have significant intrinsic resistance to many antibiotics, and additional resistance can easily develop.
(T. Lillebæk, A. Koch, H.J.N. Lorentsson, D.B. Folkvardsen, E. Svensson, Department of Tuberculosis and Mycobacteria)