No 37 - 2014
Advice concerning vaccination reminder letters
HIV 2013
Advice concerning vaccination reminder letters
Since May, Statens Serum Institut has sent out reminders to 22,000 parents of children who lack at least one vaccination under the childhood vaccination programme at 2, 6½ and 14 years, according to the Danish Vaccination Register.
The SSI is currently receiving many calls from parents whose children have, in fact, received correct vaccination both according to the yellow vaccination card and/or according to their doctor's records. In these cases, the reminder was typically sent out because one or more of the vaccinations had not been settled with the Region, as it is the settlements that form the basis for the vaccination information in the vaccination register and therefore also for the reminders.
Generally, Statens Serum Institut does not provide advice over the phone to citizens concerning the reminder scheme. Parents to children who are 2 and 6½ years old and who have been vaccinated correctly can be referred to the SSI website www.ssi.dk/vac where they can see for themselves which vaccinations have not been registered in the vaccination register; and, if they so prefer, they can also register any lacking vaccinations to the Joint Medicine Card (Danish: Fælles Medicinkort) at www.fmk-online.dk. Parents to children who are 14 years old and who have been vaccinated correctly are not required to do anything and they will not receive any further notifications.
In case of lacking settlement, it is not necessarily the vaccination marked as lacking that has not been settled correctly. It may also be one of the vaccinations given previously. For instance, if a child lacks MMR2 according to the vaccination register and the reminder, and the child has received both the MMR1 and the MMR2 according to the yellow card or the GP’s records, then the reminder may be due to lacking settlement of the MMR1 or the MMR2.
Health personnel can see the children's vaccination information at www.fmk-online.dk, and they may also register any lacking vaccinations to make sure the information in the vaccination register is in line with the information on the yellow vaccination card and/or the doctor’s records.
Health personnel may find more information on the reminder scheme at www.ssi.dk/vac and in EPI-NEWS 20/14. Health personnel may contact the Department of Infectious Disease Epidemiology by phone on 3268 3037 for advice on how to adapt the vaccinations given to children to bring them in line with the childhood vaccination programme.
As follow-up to the experiences made over the past months, the SSI will introduce minor changes in the way reminders are generated and worded.
(T. G. Krause, Department of Infectious Disease Epidemiology)
HIV 2013
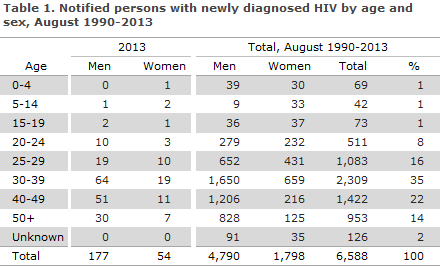
2013 saw a total of 231 notified cases of HIV, 177 men and 54 women.
The median age was 37 years for men (range 5-73 years) and 33 years for women (range 4-69 years), Table 1.
Among the 231 notified cases, 44 had previously been diagnosed with HIV abroad. Among the 44 (25 men and 19 women) persons, 3 were cases of mother-to-child transmission (MTCT), 15 were homosexually infected (MSM), 20 were heterosexually infected (HTX), 3 were infected via IV drug use (IDU) and in 3 cases the mode of infection was unknown.
Furthermore, 8 tourists were notified, 5 men and 3 women; 4 were MSM and 4 were HTX.
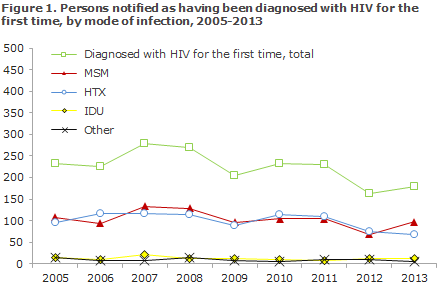
Among the 179 (147 men and 32 women) who were diagnosed with HIV for the first time, a total of 109 (61%) were Danes (including 2 second-generation immigrants) and 70 (39%) were immigrants. A total of 97 were MSM, 67 HTX and 11 IDU. Four were notified with Other or Unknown modes of infection, Figure 1
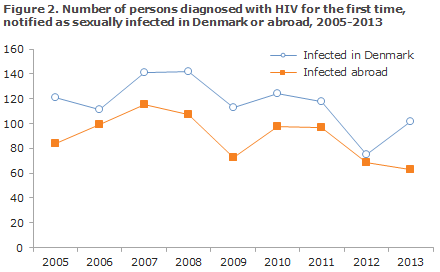
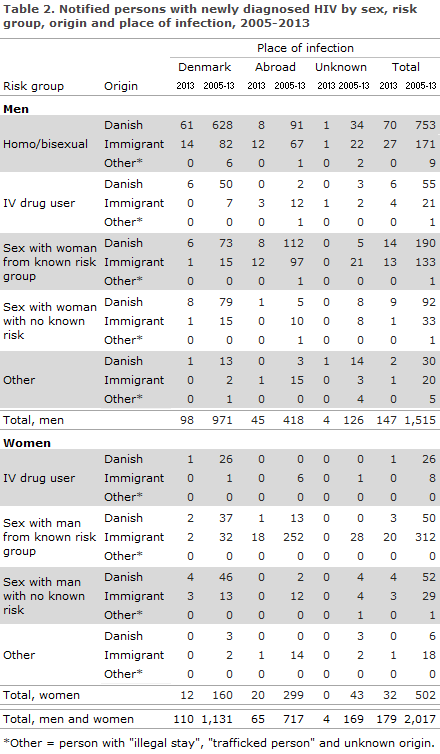
A total of 110 (62%) were infected in Denmark and 65 (36%) abroad. In 4 cases (2%), the country of infection was not stated. Figure 2 presents the distribution by notified, sexually transmitted cases in Denmark and abroad in the 2005-2013 period. The distribution by mode and place of infection is presented in Table 2.
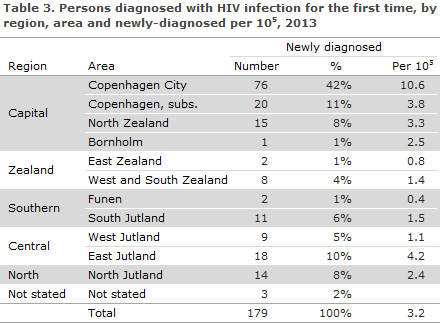
A total of 112 (63%) resided in the Capital Region of Denmark, Table 3
Among the 70 immigrants, 26 (37%) were from Sub-Saharan Africa, 21 (30%) from Europe incl. Russia, 10 (14%) from Southeast Asia, 9 (13%) from the Middle East including Afghanistan and Pakistan, 3 (4%) from South America and 1 (2%) from Greenland.
Perinatally infected persons
Two children (a boy and a girl) aged 5 and 12 years, respectively, were notified as perinatally infected; both had African mothers. One of the children was tested at the Checkpoint (The Danish AIDS Foundation's test site for MSM and immigrants, where you can be tested for HIV and syphilis without scheduling an appointment and will get the results immediately), and there was no information that the child had been tested previously; the other child was tested at a paediatric department due to symptoms.
Danish men
Of the 101 Danish men, 70 (69%) were MSM, 61 (87%) of whom had been infected in Denmark. A total of 23 (23%) were HTX, including 9 (9%) who were infected abroad (7 in Thailand, 1 in Africa and 1 in Europe). Six (6%) were infected via IDU in Denmark. In 2 cases, the mode of transmission was not stated.
Danish women
Seven of 8 Danish women were infected in Denmark and 1 in Africa. Seven were heterosexually infected, includ-ing 2 who had become infected by a bisexual partner. One was infected via IDU.
Immigrant men
Of the 46 immigrant men, 27 (59%) were MSM, 14 (52%) of whom had been infected in Denmark. A total of 14 (30%) were HTX, of whom 2 (1%) were infected in Denmark. Four (9%) were infected via IDU, 3 abroad and in one case the country of infection was not stated. Additionally, one immigrant child who was described above in the section Perinatally infected persons.
Immigrant women
A total of 24 immigrant women were notified with HIV. Of these, 23 were infected via HTX, including 5 (22%) in Denmark. Five women (21%) were detected via the pregnancy screening programme, EPI-NEWS 22-23/14. Addi-tionally, 1 immigrant child who was described above in the section Perinatally infected persons.
CD4 count at diagnosis
Among the 179 notified persons who had an address in Denmark and who were diagnosed with HIV for the first time, information on CD4 count at the time of diagnosis was available for 165 (92%). In the remaining 14 cases, CD4 counts were unavailable.
The CD4 count is a marker that indicates how the HIV virus affects the cellular immune response. A CD4 count below 350 cells per µl blood is currently indication for initiation of HAART treatment in Denmark if the patient has not wanted to initiate such treatment earlier.
Among the 165 for whom the CD4 count was stated, there were 85 (52%) whose CD4 count was below 350 cells per µl at their diagnosis, including 7 persons assessed as newly-infected based on primary HIV disease and/or a recent negative HIV test, whereas 80 (48%) had CD4 counts of 350 or above.
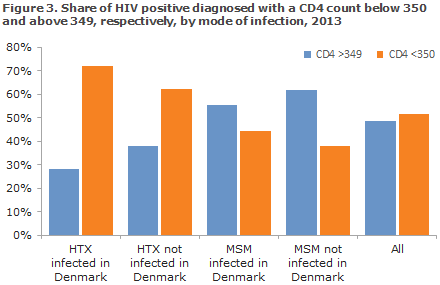
There was considerable difference in the distribution across the various infection groups. Among MSM, the share with CD4 counts >349 at diagnosis was 57% in contrast to HTX for whom the corresponding share was 34%. Figure 3 shows the distribution of CD4 counts by infection group.
AIDS
Among 179 newly-diagnosed persons, 25 (14%) were concurrently diagnosed with AIDS.
An additional 12 persons were notified with AIDS; 3 had been diagnosed with HIV within the past year, 3 had been diagnosed with HIV 1-6 years earlier and 4 had been diagnosed with HIV more than 6 years earlier. In 2 cases, the year of HIV diagnosis was unknown.
Checkpoint
A total of 21 of the 179 persons notified as being diagnosed with HIV for the first time (12%) had tested positive at the Checkpoint. Among these were 20 MSM, corresponding to 21% of the 97 MSM notified persons in 2013. Among the 20 MSM who tested positive at the Checkpoint, 14 (70%) had CD4 counts exceeding 350. An addi-tional 3 MSMs tested positive at the Checkpoint. One was a tourist who subsequently had the test confirmed in his home country. The two others have not presently been notified.
Transmitted resistance in persons with newly diagnosed HIV
In 2013, the Section for Virology Surveillance and Research diagnosed 12 new cases of transmitted, resistant HIV, corresponding to 9% of all the tested newly diagnosed patients (129). The rate of transmitted resistance has followed a decreasing trend from 9% in 2009 to 4% in 2012, EPI-NEWS 44/13.
In 2013, resistance mutations were distributed on all of the three primary treatment groups receiving Highly Active Anti-Retroviral Therapy (HAART): 3.9% (5 patients) non-nucleoside reverse transcriptase inhibitors (NNRTI), 1.6% (2 patients) nucleoside inhibitors (NRTI) and 4.7% (6 patients) protease inhibitors (PI). In 0.8% (1 patient), both NNRTI and NRTI mutations were found.
The statement comprises all newly diagnosed HIV patients who are referred to a department of infectious dis-eases and have a genotypic resistance test performed within a year after diagnosis and prior to treatment initia-tion. Between 40% and 50% of the newly diagnosed persons are every year enrolled in this study, correspond-ing to approximately 120 patients annually. Since the study was initiated in 2001, HIV sequences from 1,925 pa-tients have been tested, and mutations causing resistance were found in 119 (6.2%) sequences.
HIV of subtype B in persons with newly diagnosed HIV
HIV of subtype B is the most frequently occurring subtype in Europe, where it is found in 66% of all HIV in-fectees. Furthermore, the occurrence of subtype B varies in Europe with various epidemiological parameters including sex, mode of infection and country of origin.
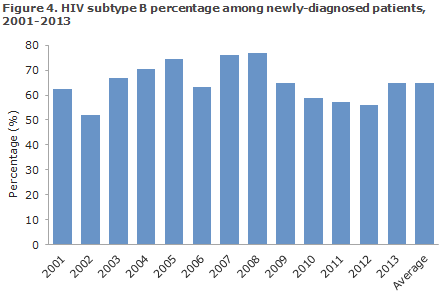
In Denmark, HIV of subtype B has been detected in 65% of all newly-diagnosed persons in the 2001-2013 period. A decrease in the occurrence of subtype B was ob-served in the 2009-2012 period, after which the occurrence increased to 65% once again in 2013.
Commentary
This year the annual HIV report is presented in a new format. Firstly, only the persons who were diagnosed for the first time have been included, i.e. persons who were diagnosed abroad and who are known to have HIV are excluded. Secondly, AIDS is no longer reported separately; it is now seen as part of the HIV condition.
These im-provements were made possible by two improvements of the notification system; first, the introduction of birth date and Soundex name code on the notifications as from 2005 and, now, the introduction of the civil reg-istration number (CPR number) in 2013. The more accurate presentation has, to some degree, come at the ex-pense of comparability with previous years' reports.
The number of reported HIV cases was slightly higher than that observed for 2012, EPI-NEWS 44/13, but, nev-ertheless, lower than the numbers recorded during the previous 8 years.
MSM and immigrants who were infected with HIV by HTX prior to their arrival to Denmark remain the primary infection groups.
The Checkpoint accounts for an ever increasing part of the notified persons. Thus, in 2013 MSM tested at the Checkpoint constituted more than a fifth of all MSM who were diagnosed in Denmark. Furthermore, it seems that MSM who are tested at the Checkpoint have their tests performed earlier in the disease course; 70% of MSM tested at the Checkpoint thus had CD4 counts exceeding 350 compared with 57% of all notified MSM.
In addition to the 2 MSM who have not been notified after testing positive at the Checkpoint, the Department of Infectious Disease Epidemiology knows of at least one person (a child) who was not notified in the course of 2013. This is worrying, because there may be more cases that have not been included in the national monitoring.
We assume that the overwhelming majority of HIV cases are notified, and the stability observed in the number of newly-diagnosed HIV positives since 2005 is striking. This applies to the absolute number as well as to the dis-tribution on infection groups.
The number of immigrants who were infected before their arrival to Denmark cannot be affected by any Danish prophylactic initiative, and the number presumably remains stable owing to a stable immigration from coun-tries with a high prevalence of HIV.
The HIV transmission that occurs in Denmark and which may therefore be changed through Danish prophylac-tic initiatives mainly occurs among MSM. The majority of European countries have seen an increase in the num-ber of newly diagnosed MSM in recent years, a trend that is not presently mirrored in Denmark.
Two factors are in play: how quickly the HIV-infected person is diagnosed and treated; and how many persons the newly infect-ed MSM transmits the condition to before being diagnosed and/or becoming less infectious, as the viral load de-creases following the initial phase which is characterised by a very high viral load.
In Denmark, an equilibrium seems to have been reached. On the one hand, the number of newly diagnosed MSM does not rise. This is seen despite the fact that there are more HIV positive MSM who could potentially increase the infection pressure, but the majority of these MSM are well-treated and therefore much less infectious.
On the other hand, the number of newly diagnosed MSM is not decreasing because the number of newly-infected, high-ly infectious MSM seems sufficient to maintain a constant infection pressure.
The number of MSM who believe that they have been infected abroad is not sufficiently high to maintain a con-stant number of newly diagnosed persons, but this number contributes to the overall picture.
(A.H. Christiansen, S. Cowan, Department of Infectious Disease Epidemiology, J. Fonager, R. Trebbien, Virology Surveillance and Research)
Link to previous issues of EPI-NEWS
10 September 2014