No 15 - 2013
Whooping cough 2011 and 2012
Whooping cough in children < 2 years
Whooping cough 2011 and 2012
This report comprises all cases of laboratory-confirmed whooping cough detected in Denmark by culture, PCR or serology in 2011 and 2012. A total of 373 cases of whooping cough were detected in 2011, whereas 2012 saw 980 cases.
In 2011 and 2012, the overall incidence was 6.7 and 17.6 per 105, respectively. The number of cases and incidence per area are shown in Table 1.

The incidence was particularly high in East Jutland both years, and in 2012 North Zealand and Funen also saw particularly high incidences.
Age and gender
Distribution by age and sex and age-specific incidence are presented in Table 2.
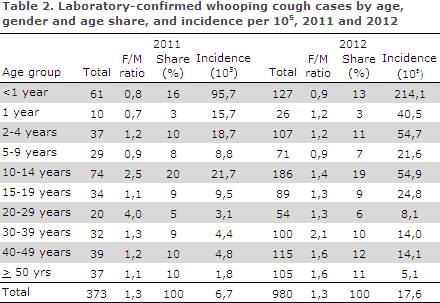
In 2012 the incidence was increased in all age-groups. In both years, the incidence was highest for the individual age groups among the 0-year olds and the 10-14-year-olds, but it was also high among the 2-4-year- olds.
The age group of 15 years and above comprised 43 % and 47 % of all detected cases in 2011 and 2012, respectively. As in previous years, there were more female than male cases among larger children and adults.
Diagnostic method
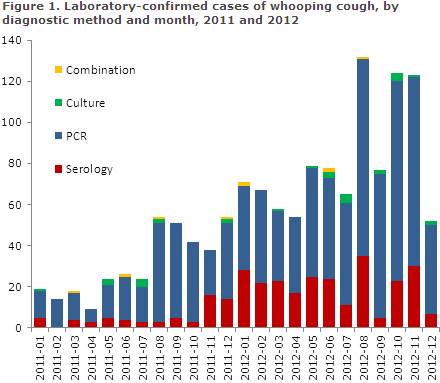
PCR testing has been the most widely used method for whooping cough diagnosis for a long period of time and 78 % and 72 % of the total number of detected whooping cough cases were detected by PCR in 2011 and 2012, respectively, Figure 1.
Serological diagnostics are gaining ground for diagnosis of adolescents and adults. The method was introduced at Statens Serum Institut at the beginning of 2010, and 29 % and 41 %, of all cases in the 15-years and above age group were detected by serology in 2011 and 2012, respectively, Figure 2.
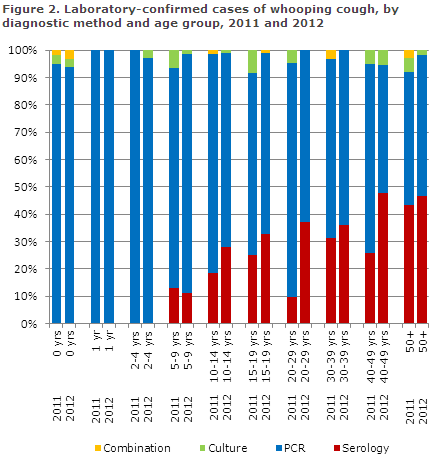
Serology can only be used to diagnose patients above 7 years of age. Culture comprised 3 % and 2 % of all cases detected in 2011 and 2012, respectively.
Commentary
The 2012 incidence was the highest observed since 2004 (24 per 105), EPI-NEWS 46/05. In the 2005-2010 period, the incidence ranged from 6 to 11 per 105. The large increase in incidence observed from 2011 to 2012 should be interpreted in view of the fact that the 2011 incidence was low and that serology gained ground in 2012, EPI-NEWS 41/12.
The introduction of the so-called SSI "Coughing Package" (serological diagnostics for whooping cough, mycoplasma and chlamydia pneumonia) in November 2011 contributed in particular to the total increase.
The increased incidence among younger children indicates that a real increase also occurred. Previously, i.e. after the introduction of acellular whooping cough vaccine in 1997, but before the introduction of the five-year booster in 2004, nearly 2,000 whooping cough cases have been detected in a single year, EPI-NEWS 44/02 and 46/05.
The increased whooping cough incidence observed in the first half of 2012 was described in EPI-NEWS 41/12 which, along with the subsequent media attention, probably encouraged the submission of samples and thus contributed to the increased number of detected cases in October and November 2012, Figure 1.
The increase, however, has since levelled off, but the current level nevertheless remains higher than levels seen in previous years.
In the three first months of 2013, a mean 46 monthly cases have been recorded, which is less than the same period in 2012, but more than in the same periods in 2010 and 2011.
Normally, a seasonal variation is observed with more cases in the second half of the year. It is important for the continued molecular-genetic monitoring of the bacterial population that culturing continues, at least to some extent.
The increasing trend is seen in most of Europe and in the US and Australia. Furthermore, a clear increase is observed in the number of whooping cough cases in larger children, adolescents and adults.
Part of this increase is owed to novel and improved diagnostic methods, but other contributing factors include increased awareness of the diagnosis and loss of vaccine-induced immunity, as the available whooping cough vaccines only provide 4-12 years of protection.
Cases in adults may cause infection of partly vaccinated or unvaccinated children. Consequently, several European countries have introduced a whooping cough booster vaccination for teenagers. This measure has, among others, been introduced in Austria, Belgium, Finland, France, Germany, Norway and Italy.
Other countries have introduced vaccination of child-bearing women. The vaccine should ideally be given in the beginning of the third semester which is considered safe for vaccination.
This measure was introduced in Great Britain, the US, Ireland and parts of New Zealand. After the vaccination, a high level of antibodies is transferred to the child, and the mother achieves optimal whooping cough protection around the time of birth.
Whooping cough is a very infectious condition, and some countries – e.g. France – have attempted to limit whooping cough infection in particularly vulnerable groups, by using a so-called cocooning strategy, where persons around the unprotected infant are offered vaccination e.g. young couples planning to become pregnant, grandparents, nursery staff and healthcare professionals who come into contact with neonates and infants.
This strategy was also employed successfully during a whooping cough epidemic in California in 2010.
It is generally considered that the current Danish vaccination programme provides good whooping cough control, but a future expansion of the programme is being contemplated in light of the observed shift in age groups following the introduction of the five-year booster vaccination in 2004 with a peak in the incidence among 10-14-year-olds, Table 2, and the increasing detection rate of whooping cough among adults which reveals a "dark figure".
(T. Dalby, Microbiology and Infection Control, P.H. Andersen, Department of Infectious Disease Epidemiology)
Whooping cough in children < 2 years
In children < 2 years of age, whooping cough is individually notifiable. Form 1515 is to be used in laboratory-confirmed cases.
2011 saw a total of 70 notified cases of whooping cough in children below 2 years of age. In 2012, the corresponding number was 155 children. Overall, 52 % were boys and 48 % girls. In 2011 and 2012, reminders were sent for 39 % and 29 % of notifications, respectively.
Small differences between the number of laboratory-confirmed and notified cases < 2 years are caused by different registration and reporting procedures at year’s end.
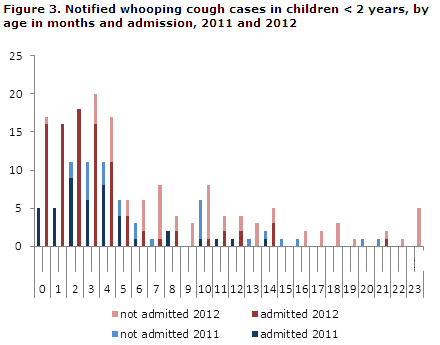
The age distribution in months for children below the age of two years is presented in Figure 3. In 2011, 62 (89 %) of the cases were below 12 months of age. Correspondingly, 2012 saw 127 (82 %) cases below 12 months of age.
Among the 70 notified children < 2 years in 2011, 32 (46 %) were unvaccinated, while three (4 %) had received three whooping cough vaccinations. In 2012, 72 of 155 children (46 %) were unvaccinated, whereas 15 (10 %) had received all three vaccinations (DTaP-IPV/Hib).
Admission and sequelae
Among the 70 notified cases in 2011, a total of 44 children (62 %) were admitted one or more times. In 2012, the corresponding number was 95 (61 %). Among the youngest, i.e. those below 3 months of age, all 21 (100 %) were admitted for one or more days in 2011, and 50 of the 51 children (98 %) were admitted in 2012.
Based on notifications and/or discharge summaries, no whooping cough deaths were recorded in this age group in 2011 and 2012, but several children were notified with pneumonia and a need for C-pap treatment.
Transmission
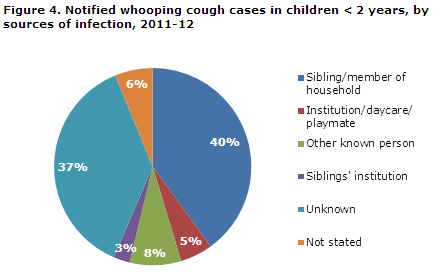
The source of infection was known for 47 % of the notified children in 2011 and for 60 % of the notified children in 2012. In 2011, siblings and other members of the household comprised 32 % of the infection sources, in 2012 this number was 43 %, Figure 4.
Infection of and by health professionals
A single case of whooping cough infection in a health professional was described in the individual notifications filed in 2012. The mother (32 years of age) of an 11-month-old child monitored another child admitted with whooping cough. She subsequently fell ill with whooping cough and later her own child was infected.
Similarly, 2012 saw the case of a 57-year-old health visitor who fell ill in August of 2012 following occupational exposure to a neonate with whooping cough. A throat swab was made and the health visitor tested positive to whooping cough.
Subsequently, the Medical Officers of Health in the region were involved in contact tracing and in disseminating information to the parents of the smaller and larger children, with whom the health visitor had come into contact with during the infectious period. No information was provided on further infection of infants or other persons.
Commentary
In 2011, the whooping cough incidence in children below two years of age was at par with that of the previous year, whereas 2012 saw a clear increase. The increase was more pronounced in the first half than in the second half of 2012.
It is unknown to which extent the increased incidence among older children and adults has affected awareness of the whooping cough diagnosis in children below two years of age.
Timely whooping cough vaccination of infants in the form of DTaP-IPV/Hib is essential as significant protection against whooping cough is only achieved after two vaccinations. The recommended vaccination times at 3, 5 and 12 months of age should be followed to the extent possible.
Furthermore, a DTaP-IPV booster is recommended at five years of age. In unvaccinated or partly vaccinated children < 2 years, who are exposed to whooping cough, antibiotic prophylaxis should be considered in accordance with the guidelines described in EPI-NYT 41/12.
Health personnel may comprise an infection risk, particularly to smaller children.
(L.K. Knudsen, P.H. Andersen, Department of Infectious Disease Epidemiology)
Link to previous issues of EPI-NEWS
10 April 2013