No 21 - 2013
The new coronavirus – MERS-CoV – still demands attention
DTaP-IPV/HIB vaccination coverage 2012
The new coronavirus – MERS-CoV – still demands attention
Healthcare professionals are encouraged to remain attentive to the new coronavirus as person-to-person transmission has now been demonstrated in families and at hospitals in European countries and on the Arabian Peninsula and nearby countries.
The WHO has coined the new virus MERS-CoV (Middle East Respiratory Syndrome Coronavirus).
If a patient meets the below criteria (case definition), GPs and emergency call service physicians should confer by phone with their local infectious medicine department to determine the need for referral for clinical assessment, isolation and sampling:
The patient shall have stayed on the Arabian Peninsula or nearby countries within the previous ten days, or within the past ten days have come into contact with a person with suspected or confirmed MERS-CoV infection
AND
have an acute and severe respiratory infection OR have another serious infection and underlying chronic disease (possibly in conjunction with immunosuppression).
Travellers to the Arabian Peninsula and nearby countries shall also remain attentive to the condition.
Travellers to the affected areas should observe standard hygiene recommendations, including good hand-hygiene, and they should avoid close contact to animals (particularly animal excretions and secretions, e.g. saliva and faeces).
It should be stressed that the risk of infection for travellers is considered to be very low and that no travel restrictions have been introduced.
For further information, see the webpage of the Danish Health and Medicines Authority, www.sst.dk.
(Department of Infectious Disease Epidemiology)
DTaP-IPV/HIB vaccination coverage 2012
Vaccination coverage was calculated as per 10 January 2013 on the basis of person-identifiable data from the national Childhood Vaccination Database.
There is a 2-3-month lag from a vaccination is performed until it is recorded in the Vaccination Database. Vaccinations administered after mid November 2012 are therefore not included in this report.
Data for the previous report on coverage at the end of 2011, EPI-NEWS 23a/12, were calculated as per 16 April 2012.
Consequently, for this reason alone, coverage at the end of 2012 may appear marginally lower.
The reported coverage provides a minimal estimate, among others because only vaccinations performed in Denmark by GPs are included. Furthermore, a certain under-reporting to the Childhood Vaccination Database has been shown, EPI-NEWS 20/12.
Method of calculation
Vaccination coverage was recorded using the administrative service codes indicated by GPs when settling the first, second and third DTaP-IPV/Hib vaccinations, EPI-NEWS 6/10 and 9/10.
In cases where GPs used the same vaccination code at all three vaccinations of the same child, the codes have automatically been changed to include the missing codes.
The numerator is therefore e.g. the number of children born in 2012 who received the initial DTaP-IPV/Hib vaccination, and the denominator is the number of children from the birth year residing in Denmark when the data were analysed.
As in previous years, the codes settled using a parent's civil registration number were ascribed to the child whose age corresponded to that recommended for the vaccination in question.
Any vaccination delay will contribute to an increase in vaccination coverage over time. Vaccination coverage for each vaccine is shown by birth cohort in Table 1 and Table 2.
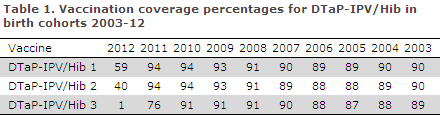
DTaP-IPV/Hib 1, 2 & 3
Among the entire 2012 birth cohort, a total of 59% had received the first and 4% the second DTaP-IPV/Hib vaccination. The lower coverage observed for these vaccinations was expected as vaccination of this cohort had not been concluded at the calculation date.
Furthermore, the earlier calculation date contributes to the lower coverages compared with the previous report, EPI-NEWS 23a/12.
In the 2003-2011 birth cohorts, a total of 89-94% had received the first, 88-94% the second and 76-91% the third DTaP-IPV/Hib vaccination.
Coverage remained at the same level from birth cohort 2003 to birth cohort 2007. As from birth cohort 2008, coverage has followed an increasing trend, primarily for the first two vaccinations.
For the 2010 birth cohort, the coverage of the first two vaccinations has increased by one and two percentage points, respectively, compared with the previous report, EPI-NEWS 23a/12.
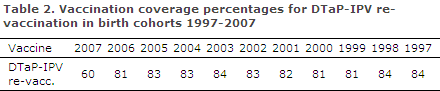
DTaP-IPV re-vaccination
Coverage for the 1997-2000 birth cohorts was 81-84% and displayed a slightly decreasing trend. For birth cohorts 2001-2005, coverage was 82-84% and followed a slightly increasing trend.
Coverage for 2005, for example, increased by two percentage points compared with the previous report, EPI-NEWS 23a/12.
The 2006 cohort now holds children aged 6-7 years who should have concluded the vaccination sequence (current coverage 81%), as re-vaccination should be administered at five years of age, whereas the 2007 cohort had expectedly not concluded the vaccination sequence at the calculation date.
National coverage
Like in previous years, DTaP-IPV/Hib 3 coverage for birth cohorts 2009-2011 and DTaP-IPV re-vaccination coverage for birth cohorts 2005-2007 was slightly lower in Copenhagen City, i.e. the municipalities of Copenhagen, Frederiksberg, Tårnby and Dragør, than in the remaining parts of Denmark, Table 3.
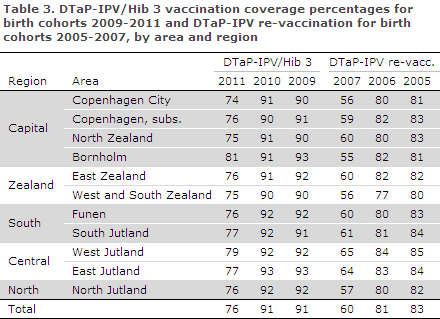
Data detailing coverage at the municipal level are available at www.ssi.dk/data as figures and map views.
It is possible to filter the data provided by gender, relevant birth years, municipality and area.
Coverage at the municipal level will be sensitive to the size of the municipality.
Commentary
Since birth cohort 2008, a slight increase has been observed in DTaP-IPV/Hib vaccination coverage at 3 and 5 months. The recorded increase is consistent, although nearly 10% of a birth cohort does not receive one or more of the three primary DTaP-IPV/Hib vaccinations.
Since birth cohort 2001, the coverage of DTaP-IPV re-vaccination has increased slightly, i.e. it has followed a trend towards a higher coverage in later birth cohorts and also a higher coverage for each birth cohort over time, e.g. birth cohort 2005, in which coverage increased by two percentage points compared with the previous report, EPI-NEWS 23a/12.
The current coverage is equivalent to about four in every five children being re-vaccinated at five years of age. Although the coverage is a minimal estimate, the DTaP-IPV re-vaccination coverage remains less than satisfactory.
Previous studies have demonstrated that vaccination coverage is lower among children of very young mothers and mothers > 30 years, children of single parents, children who have many siblings and children of non-Danish origin, EPI-NEWS 20/11.
Furthermore, vaccination coverage in Copenhagen is lower than that observed in the rest of Denmark. This observation has also been made for other vaccines; yet, we have no clear explanation why this is so.
Healthcare professionals should be particularly attentive to ensure vaccination coverage in these groups and areas.
(P.H. Andersen, L.K. Knudsen, P. Valentiner-Branth, Department of Infectious Disease Epidemiology)
Link to previous issues of EPI-NEWS
22 May 2013