No 19/22a - 2026
Human cases of hantavirus in Denmark, 2010–2025
Human cases of hantavirus in Denmark, 2010–2025
Hantavirus is a group of zoonotic viruses comprising more than 60 species, each occurring in specific geographical regions of the world. Human infection may occur through inhalation of virus particles from the urine, faeces or saliva of infected rodents, and transmission is often associated with particular rodent species. Andes hantavirus, which caused an outbreak on a cruise ship in spring 2026, is the only known hantavirus species capable of human-to-human transmission. This species does not occur in Denmark.
In Denmark, Puumala hantavirus is responsible for most infections. The bank vole (Myodes glareolus) serves as the reservoir. Bank voles are found throughout Denmark, but human infections with Puumala hantavirus are most frequently identified in south-eastern Funen, particularly in the coastal area from Svendborg to Nyborg and around Glamsbjerg. A few cases have also been detected south of Silkeborg in Jutland. A hantavirus species known as Saaremaa hantavirus has also been detected in Denmark, but it is very rare. Saaremaa hantavirus is found in the striped field mouse (Apodemus agrarius), which has established populations on the islands of Lolland and Falster, but has also been observed sporadically on Fejø, Femø, in Central Jutland, and on Zealand.
The occurrence of human hantavirus infection is influenced by the size of the bank vole population, which may vary from year to year. Larger populations may be observed following so-called mast years, when forests produce particularly large quantities of acorns and beechnuts.
Infection with Puumala and Saaremaa hantavirus may lead to a mild form of haemorrhagic fever with renal involvement, known as nephropathia epidemica (NE), which in severe cases may result in acute renal failure requiring dialysis. The disease course is typically characterised by an initial febrile phase with influenza-like symptoms, headache, and flank or abdominal pain, followed by varying degrees of hypotension and oliguric renal failure. Laboratory findings often include mild leukocytosis, elevated CRP, thrombocytopenia and hyponatraemia. Microscopic haematuria and marked albuminuria are also common. Treatment is symptomatic and the prognosis is generally good.
A laboratory-confirmed case is defined by detection of hantavirus RNA in blood, respiratory material or urine and/or detection of both hantavirus IgM and IgG antibodies in blood, or by initial detection of hantavirus IgM antibodies followed by IgG seroconversion in a later blood sample.
For the Danish hantavirus species, antibody testing is particularly important because the viraemic phase is often over when patients develop NE, whereas hantavirus RNA testing may be relevant for other hantavirus species, such as Andes hantavirus.
Isolated detection of hantavirus IgM antibodies is considered a possible case of hantavirus infection or a false-positive result. If clinical suspicion persists, repeat antibody testing after 1–2 weeks is recommended. IgG seroconversion confirms infection.
Routine hantavirus species identification is not performed in Denmark. Since November 2023, hantavirus has been laboratory-notifiable from diagnostic laboratories to SSI.
For a more detailed description of symptoms, prevention, treatment and diagnostics, please refer to the hantavirus disease dictionary.
Detected human cases of hantavirus in Denmark, 2010–2025
Diagnostic test results for human hantavirus infections in Denmark were extracted from the Danish Microbiology Database (MiBa) for the period from January 1, 2010 to December 31, 2025.
The Department of Clinical Microbiology at Odense University Hospital performed 75% of hantavirus diagnostics during the study period, while 21% of samples were analysed at Statens Serum Institut (SSI) and 4% at the Department of Clinical Microbiology, Aarhus University Hospital Skejby, where hantavirus diagnostics were discontinued in 2013.
During 2010–2025, a total of 168 laboratory-confirmed human cases of hantavirus infection were recorded in Denmark. The number of cases per year is shown in Figure 1. The annual number generally ranged between 5 and 15 cases, varying from 2 cases in 2013 to 23 cases in 2012.
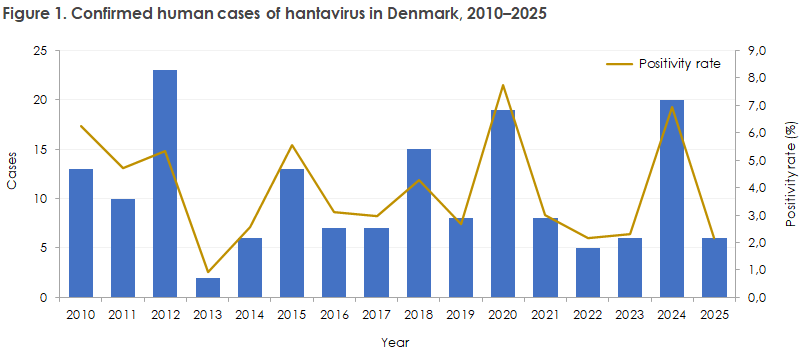
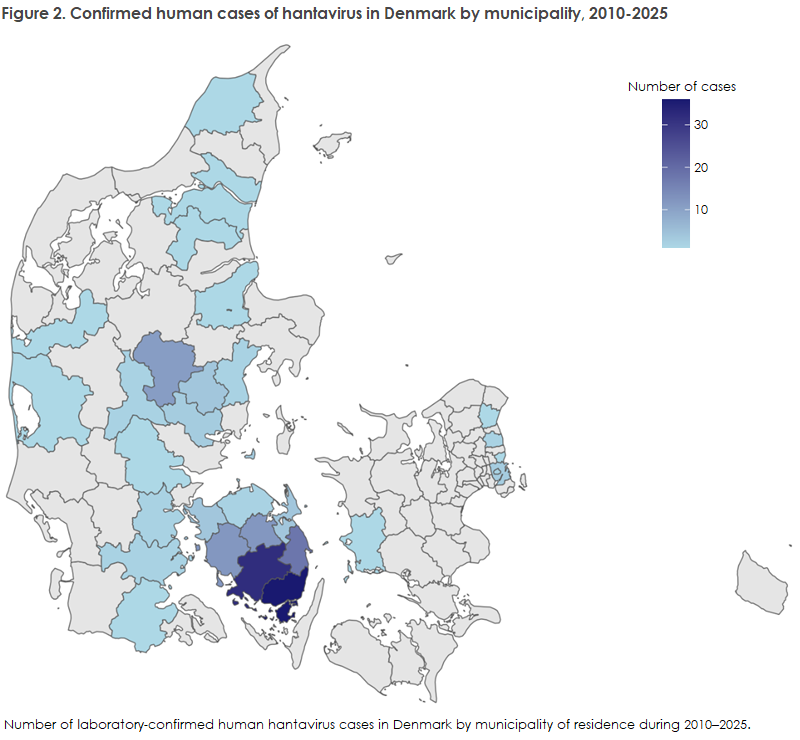
Figure 2 shows the geographical distribution of confirmed cases by municipality of residence at the time of first sampling. A clear concentration of cases is observed in municipalities in southern Funen. Additional clusters are seen in Central Jutland, together with sporadic cases in North Jutland, Southern Jutland and Zealand.
During the study period, 93 possible cases with isolated detection of hantavirus IgM antibodies were recorded. These were not included in this report because of the possibility of non-specific reactions and false-positive results. Further clarification of possible cases would require systematic correlation with clinical information, which was not possible to do for this overview.
Comment
Hantavirus has recently received increased attention following an outbreak involving Andes hantavirus on a cruise ship in the Atlantic Ocean. Andes hantavirus may cause severe cardiopulmonary syndrome and occurs primarily in South America. SSI is currently monitoring the outbreak, read more here.
As described above, only a small number of human hantavirus cases are detected in Denmark each year, approximately 5–15 cases annually, and these usually present as relatively mild disease.
However, not all infected patients are tested for hantavirus, and the true number may therefore be higher. Furthermore, information on possible infection acquired during travel abroad was not included in the present analysis.
The hantavirus species found in North and South America typically cause cardiopulmonary syndrome, whereas hantavirus species found in south-eastern Europe and Asia more often cause haemorrhagic fever with renal syndrome, which generally results in more severe disease than infections caused by the Puumala and Saaremaa hantaviruses occurring in Denmark.
In a Danish context, hantavirus infection should be considered as a differential diagnosis in patients with acute renal failure, thrombocytopenia and possible exposure to bank voles, for example after sweeping a garage, cleaning a garden shed or similar activities.
Among patients with a travel history, other hantavirus species may occur. Clinicians should therefore be aware of the disease course and obtain relevant exposure and travel histories. Due to the particular risk of person-to-person transmission associated with Andes hantavirus, the Danish Health Authority has recently prepared national guidelines for the management of Andes hantavirus.
These guidelines describe the management of suspected and confirmed cases, including diagnostics, treatment, infection prevention measures and contact management.
(A.V. Søndergaard, P. Valentiner-Branth, P.H. Andersen, L.S. Vestergaard, Department of Infectious Disease Epidemiology and Prevention; U.V. Schneider, B.B. Jensen, Virology and Microbiological Preparedness; R.R. Schmidt-Nielsen, M. Volstedlund, Data Integration & Analysis, Statens Serum Institut; N.S. Andersen, T.G. Jensen, Department of Clinical Microbiology, Odense University Hospital; M.K. Thomsen, Department of Clinical Microbiology; I.K. Ystrøm, Department of Nephrology, Aarhus University Hospital)