No 13 - 2024
Parvovirus B19 and pregnancy
Parvovirus B19 and pregnancy
Currently, an increase is being observed in the number of Fifth disease cases in Denmark. The Fifth disease is caused by parvovirus B19 infection. Fifth disease is not notifiable, and its prevalence is therefore not monitored systematically by Statens Serum Institut (SSI). After being notified by obstetricians of an increased occurrence of pregnant women with Fifth disease, the SSI has calculated the number of laboratory-verified Fifth disease cases over the past ten years. Concurrently, increased online search activity for parvovirus B-19 infection, transmission and pregnancy has been registered, witnessing increased popular interest.
Fifth disease occurs all of the world and is most frequently a mild childhood disease. Following parvovirus infection, the infected person achieves life-long immunity. Fifth disease, also known as erythema infectiosum or slapped cheek syndrome, typically runs a two-phased course, starting with catarrhalia and light fever. Subsequently, children often develop a red rash on the cheeks, giving rise to the name slapped cheek syndrome. Often adults do not develop the rash, but occasionally they do develop joint pain. In 20-30% of cases, the infection is asymptomatic. In rare cases, parvovirus B19 infection may cause serious disease in pregnant women and immunosuppressed individuals. Generally, parvovirus rarely causes disease that requires hospitalisation.
Parvovirus B19 occurrence in Denmark
In Denmark, it is estimated that approx. 60% of adults have had B19 infection and are therefore immune to re-infection. Parvovirus B19 infections occur endemically all year, and epidemics occur approx. every 3-4 years, typically in the spring months. According to previous Danish studies, the infectious pressure in the population is approx. 13% (seronegative pregnant women) during epidemics and around 1.5% in non-epidemic periods.
The most recent parvovirus epidemic occurred in 2017 when a total of 671 persons with parvovirus B19 infection were identified in the MiBa. Among these, 102 (15%) were pregnant women, of whom 15 were hospitalised, corresponding to 15%. The number of persons with detected B19 infection currently follows an increasing trend compared with previous years. As presented in Figure 1, the number of B19 infections is currently on a par with that recorded in 2017. To date, a total of 250 cases have been detected in 2024, among which 50 (20%) were pregnant women with parvovirus. Five of the 50 women, corresponding to 10% of the pregnant women, were hospitalised.
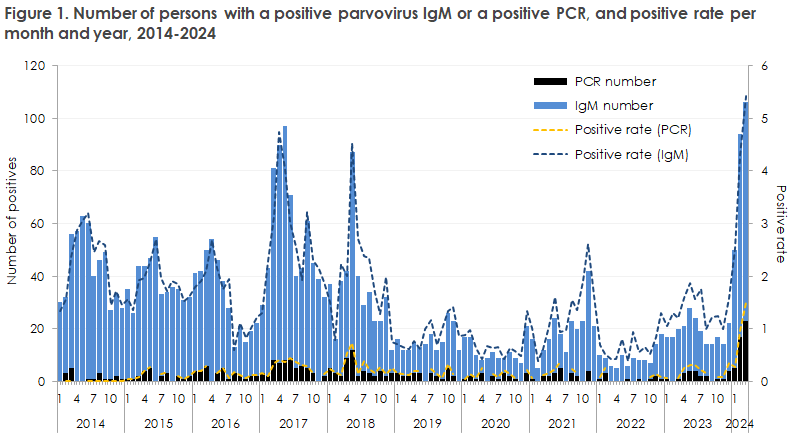
The 2024 number is expected to keep climbing, and the level may slightly exceed that observed in 2017 due to a lower occurrence of parvovirus B19 infections during the COVID-19 pandemic. An increase is also seen in the share of positive tests (i.e. positive rate) compared with previous years and months. In March 2024, the positive rate is 5.4% for IgM and 1.5% for PCR tests, which is 2 and 4.5 times higher than in March 2017. The positive rate is calculated based on a single positive test per person, but may comprise several negative tests per person.
Risk for the foetus
If a seronegative woman becomes infected, the infection will generally be insignificant, but a 25% probability exists that the foetus is infected, typically four weeks after the mother has become infected, even though transmission intervals as long as three months have been reported. The risk of transmission increases throughout pregnancy but hardly ever has any consequences for the child when the infection occurs after week 20. If a seronegative pregnant woman becomes infected before her 20th gestational week, the infection will generally be insignificant, but in rare cases it may cause spontaneous abortion, hydrops foetalis and foetal death. Among the total number of cases of foetal death/abortion in Denmark, cases associated with parvovirus B19 infections constitute a very small share (approx. 0.1-0.8%). There is no risk of congenital malformation in live-born children.
Infection and prophylaxis
The virus is transmitted through droplets and via blood or vertically from mother to foetus. Transmission requires close contact and may, to some extent, be prevented through good hand hygiene.
The incubation period is approx. 1-2 weeks. The risk of infection is largest early in the disease course, which is characterised by fever and mild airway symptoms. Once the rash has presented, mainly in children, the disease is no longer infectious. Targeted prophylaxis is difficult as the disease may be transmitted before symptom onset and because it may present with only mild symptoms that are similar to those of other viral infectious diseases. No vaccine is available for parvovirus B19 infection.
Previous Danish studies have shown that the risk of infection among pregnant women is larger among women who have children and that the risk increases with the number of children in the home, which illustrates that the risk of infection is higher in homes with children. With respect to routes of infection, it seems that approx. 50% are infected by household contacts, and 20-30% occupationally.
Diagnostics
Parvovirus B19 infection may be diagnosed by detection of virus in the blood via PCR or by detection of specific IgM and IgG antibodies. Among pregnant women, parvovirus testing is normally limited to cases with specific exposures or disease signs. Pregnant women with parvovirus B19 infection are referred to an obstetric department for weekly foetal ultrasound scans to test for anaemia and, in some cases, PCR testing of amniotic fluid in the foetus.
Current guidelines
In Denmark, pregnant women are not screened routinely for parvovirus B19 antibodies. The Danish Health Authority has assessed that the value of affording the pregnant woman a right of absence from work due to the risk to the child is very limited. Consequently, the Danish Health Authority does not recommend that pregnant women are afforded such absence due to parvovirus B19 infection in their surroundings, unless extraordinary causes support such a measure (e.g. blood condition in the mother).
(A.C. Nordholm, F. T. Møller, M. Wessman, T. Funk, B. Kristensen, U. Jeyaratnam, Department of Infectious Disease Epidemiology and Prevention, J.E. Mollerup, A. Moltke-Prehn, S.F. Ravn, L.F. Sørensen and R.T. Nielsen, Department of Data Integration and Analysis)
22 March 2024