No 45 - 2015
Mandatory registration of vaccinations in electronic vaccination Card
Increase in the number of detected Mycoplasma pneumoniae infections
Mandatory registration of vaccinations in the Danish Vaccination Register
In pursuance of Executive Order on Access to and Registration etc. of Medicinal Product and Vaccination Information of 8 May 2014, all physicians shall report any vaccinations in the Danish Vaccination Register (DVR) as from 15 November 2015. Henceforth, all vaccinations, including travel vaccinations, influenza vaccinations administered at work sites and the like shall be registered.
Mandatory registration applies to all physicians, including those affiliated with medical practices, hospitals and vaccination clinics. Registration shall be performed as part of current treatment of any citizen. Physicians may authorise assistants to view and register vaccinations on their behalf. Registration may either be done via www.fmk-online.dk or by integrating the Danish Vaccination Register (DVR) into the electronic health record system used by the physician. For more information about the current state of integration of the DVR into the health record systems used in medical practices, please see here (in Danish language).
Vaccinations that are settled with the Region (e.g. childhood vaccinations and influenza vaccinations for risk groups) will continue to be imported automatically into the DVR. If a childhood vaccination which was initially reported directly in the DVR is subsequently settled with the Region and therefore imported into the DVR with delay, the two registrations will be linked through information about the person, the vaccine and the vaccination date, to avoid repeat registrations of the same vaccination.
Vaccinations need to be reported directly to the DVR to achieve an up-to-date overview of the administered vaccinations as settlements with the Region are imported with up to 3 months of delay. Additionally, direct registration in the DVR also means that information on batch number and product name will be available, and this information is important in the monitoring of the safety and effect of vaccinations.
For more information about the DVR, including about how vaccinations may be registered, please see here
(T.G. Krause, Department of Infectious Disease Epidemiology, L. Ærbo, H. Balle, the Danish Health Data Authority)
Increase in the number of detected Mycoplasma pneumoniae infections
Epidemics of airway infections caused by Mycoplasma pneumoniae (MP) are normally observed at 4-6-year intervals. In 2010 and 2011, an epidemic persisted for 2 autumn and winter seasons, EPI-NEWS 48/10 and 41/11 and also Figure 1. Outside of epidemic periods, a limited number of cases are normally seen in the summer, followed by an increase in numbers in the course of the autumn/winter, as was the case in 2014, Figure 1.
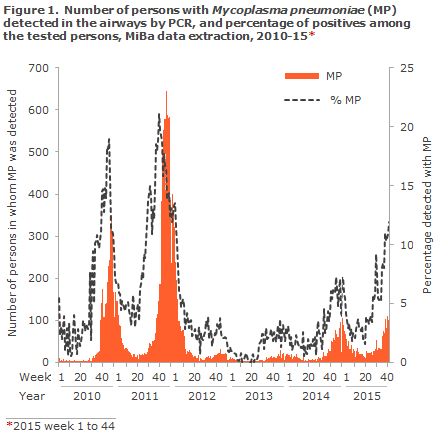
Since mid-September 2015, data on national laboratory results extracted from the Danish microbiology database (MiBa) have shown a considerable increase in the number of weekly airway samples that test positive for MP by PCR, increasing from approx. 30 cases in the weeks 30-37 to approx. 100 cases in weeks 41-44. In the same period, the percentage of positives rose from approx. 5% to 11%. In the past month, more than twice as many MP infections have been detected as in the same period last year. The increase has been observed in nearly all parts of Denmark, but is less pronounced in the Region of Southern Denmark. About 50% of the detected infections occur in children below 18 years of age, and 24% in the 7-12-year-old age group. It is characteristic that MP infections occur among younger school children.
The MP infection presents gradually with influenza-like symptoms, but only a limited temperature increase. In a short space of time a dry, irritating cough (bronchitis) presents which is typically aggravated when the patient is lying down. Frequently, patients complain of a burning pain behind the sternum when coughing. The cough may extend in time, e.g. for 1-2 months or longer.
Only a small minority develop genuine pneumonia, and MP infections are frequently so mild that no treatment is needed. In case of fever and/or pneumonia, antibiotics may be given. An early diagnosis may be made through detection of MP in swabs from the upper airways or in airways secretions by gene amplification technique (e.g. PCR). The diagnosis may also be made by detection of an increase in titres in antibodies against MP. Usually, a few weeks pass before antibodies can be detected.
It is currently too early to decide if we are facing a minor autumn cluster of MP infections or an incipient epidemic. Experience shows that an increase from approx. 5% positives to >15 % positives in the course of some weeks indicates that an epidemic is in course. The situation will be monitored in weeks to come.
(Søren Uldum, Microbiology and Infection Control, H-D. Emborg, T.G. Krause, Department of Infectious Disease Epidemiology)
Link to previous issues of EPI-NEWS
4 November 2015